OHIO - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated March 15th, 2017
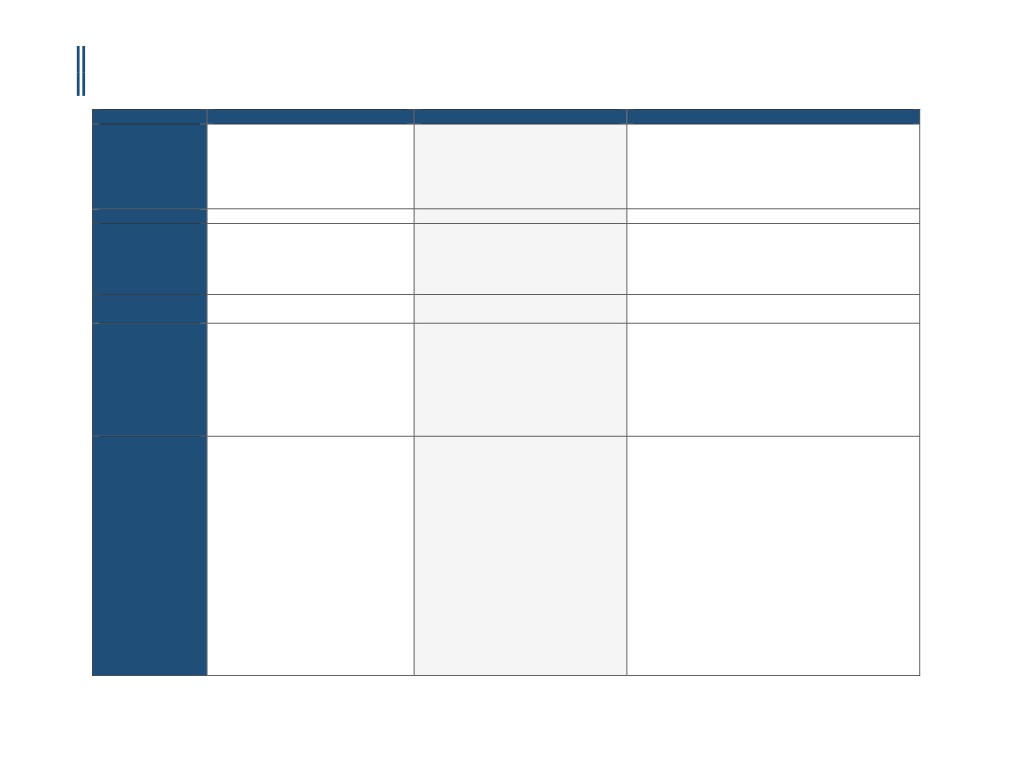
Payer
Anthem BlueCross
Medical Mutual of Ohio
Aetna
Policy Name
Coronary Artery Imaging: Contrast-
Computed Tomography and Angiography
Cardiac CT, Coronary CT Angiography and Calcium Scoring
Enhanced Coronary Computed
of the Heart and Coronary Arteries
Tomography Angiography (CCTA),
Coronary Magnetic Resonance
Angiography (MRA), and Cardiac
Magnetic Resonance Imaging (MRI)
Policy #
RAD.00035
N/A
0228
RBM
AIM Specialty Health® (AIM)
eviCore (Product line and POS dependent)
customized fax forms posted on the
Documentation Standards, Forms and
Policies page
Applicable CPT
75574
75571 75572 75573 75574
Code(s)
Applicable ICD
Not Listed
E08.00 - E09.9
Code(s)
E10.10 - E13.9
I37.0 - I37.9
M30.3
Q21.3
Q26.0 - Q26.9
Q87.40 - Q87.43
R94.39
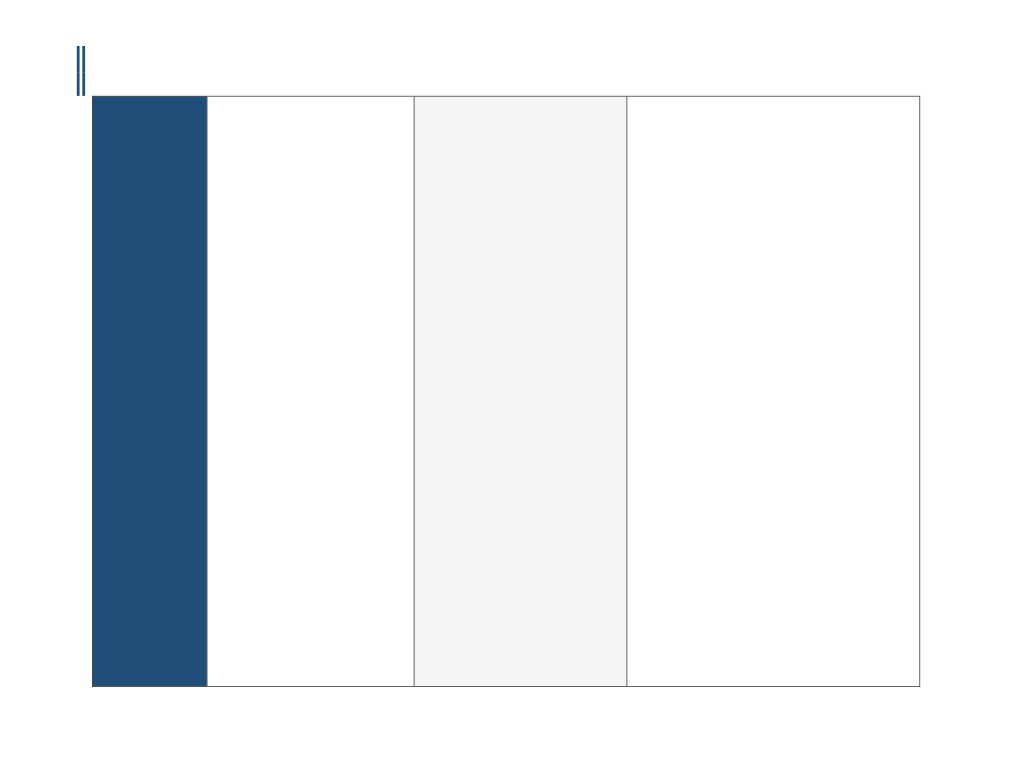
Covered
Contrast-enhanced coronary computed
Medical Mutual of Ohio has not made
I.
Aetna considers cardiac computed tomography (CT)
tomography angiography (CCTA),
their Coronary CT medical policy public.
angiography of the coronary arteries using 64-slice or
coronary magnetic resonance
greater medically necessary for the following indications:
angiography (MRA), or cardiac magnetic
Registered providers may view the
A.
Rule out significant coronary stenosis in persons
resonance imaging (MRI) is considered
with a low or intermediate pre-test probability of
medically necessary for the evaluation of
website that allows providers and their
coronary artery disease or atherosclerotic
suspected anomalous coronary arteries:
staff access to coding information, clinical
cardiovascular disease by Framingham risk scoring,
o In pediatric individuals (age < 18
guidelines, and disease management
Pooled Cohort Equations, or by American College of
years) either before or after
tools.
Cardiology (ACC) criteria (see Appendix), with any of
conventional angiography; or
the following indications:
o In adults (age 18 and over) when
1. Evaluation of persons with chest pain who cannot
conventional angiography has
perform or have contraindications to exercise and
been unsuccessful or has provided
pharmacological stress testing (see Appendix); or
equivocal results and the results
2. Evaluation of persons with chest pain presenting to
could impact treatment.
the emergency department in persons without acute
ECG changes or positive coronary markers when an
imaging stress test or coronary angiography are being
1
CCM-100-131-A
OHIO - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated March 15th, 2017
deferred as the initial imaging study.
B. Rule out significant coronary stenosis in persons with a
low pre-test probability of coronary artery disease or
atherosclerotic cardiovascular disease by Framingham
risk scoring, Pooled Cohort Equations, or by American
College of Cardiology (ACC) criteria (see Appendix) with
a positive (i.e., greater than or equal to 1 mm ST
segment depression) stress test.
C. Evaluation of asymptomatic persons at an
intermediate pre-test probability of coronary heart
disease or atherosclerotic cardiovascular disease by
Framingham risk scoring or Pooled Cohort
Equations (see Appendix) who have an equivocal or
uninterpretable exercise or pharmacological stress
test. Note: Current guidelines from the American Heart
Association recommend against routine stress testing
for screening asymptomatic adults.
D.
Pre-operative assessment of persons scheduled
to undergo 'high-risk" non-cardiac surgery, where an
imaging stress test or invasive coronary angiography is
being deferred unless absolutely necessary. The ACC
defines high-risk surgery as emergent operations,
especially in the elderly, aortic and other major
vascular surgeries, peripheral vascular surgeries, and
anticipated prolonged surgical procedures with large
fluid shifts and/or blood loss involving the abdomen
and thorax.
E. Pre-operative assessment for planned non-coronary
cardiac surgeries including valvular heart disease,
congenital heart disease, and pericardial disease, in lieu
of cardiac catheterization as the initial imaging study.
F. Detection and delineation of suspected coronary
anomalies in young persons (less than 30 years of age)
with suggestive symptoms (e.g., angina, syncope,
arrhythmia, and exertional dyspnea without other
known etiology of these symptoms in children and
adults; dyspnea, tachypnea, wheezing, periods of
pallor, irritability (episodic crying), diaphoresis, poor
feeding and failure to thrive in infants).
G.
Calculation of fractional flow reserve (HeartFlow
FFRCT) for persons with stable, recent onset chest pain
2
CCM-100-131-A
OHIO - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated March 15th, 2017
of suspected cardiac origin and a clinically determined
intermediate (10% to 90%) risk of coronary artery
disease.
II. Aetna considers CT angiography of cardiac morphology
for pulmonary vein mapping medically necessary for
the following indications:
A.
Evaluation of persons needing
biventricular pacemakers to accurately identify the
coronary veins for lead placement.
B.Evaluation of the pulmonary veins in persons
undergoing pulmonary vein isolation procedures for
atrial fibrillation (pre- and post-ablation procedure).
III. Aetna considers CT angiography medically necessary
for preoperative assessment of the aortic valve annulus
prior to anticipated transcatheter aortic valve
replacement (TAVR).
IV. Aetna considers cardiac CT for evaluating cardiac
structure and morphology medically necessary for the
following indications:
A.
Anomalous pulmonary venous drainage;
B. Evaluation of other complex congenital heart diseases;
C. Evaluation of sinus venosum atrial-septal defect;
D.
Kawasaki's disease;
E. Person scheduled or being evaluated for surgical repair
of tetralogy of Fallot or other congenital heart diseases;
F. Pulmonary outflow tract obstruction;
G.
Suspected or known Marfan's syndrome.
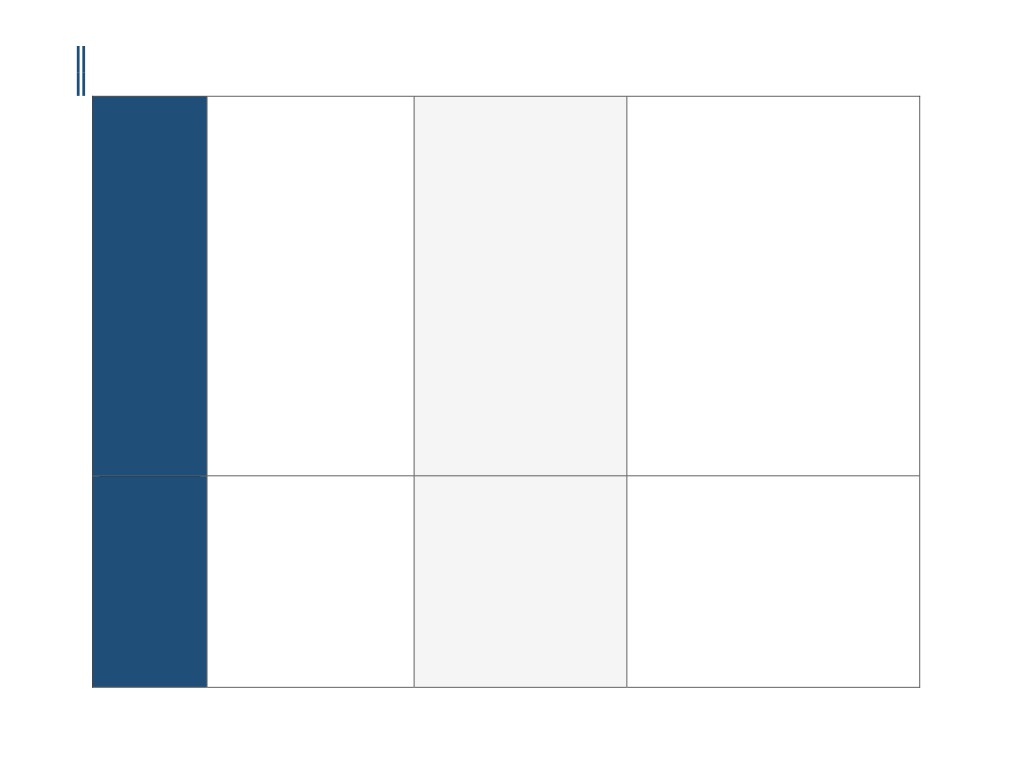
Not Covered /
•
Coronary computed tomography
I.
Aetna considers cardiac CT angiography experimental
Investigational and
angiography (CCTA) or coronary
and investigational for persons with any of the following
Not Medically
magnetic resonance angiography
contraindications to the procedure because its
Necessary
(MRA) is considered investigational
effectiveness for indications other than the ones listed
and not medically necessary for all
above has not been established:
other indications, including, but not
A.
Body mass index (BMI) greater than 40.
limited to, the following:
B. Inability to image at desired heart rate (under 80
o Screening for coronary artery
beats/min), despite beta blocker administration.
disease (CAD), either in
C. Person with allergy or intolerance to iodinated
asymptomatic individuals or as
contrast material
part of a preoperative evaluation;
D.
Persons in atrial fibrillation or with other
or
significant arrhythmia.
o Diagnosis of CAD, in individuals
E. Persons with extensive coronary calcification by plain
with acute or non-acute
film or with prior Angston score greater than 1,700.
3
CCM-100-131-A
OHIO - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated March 15th, 2017
symptoms, or after a coronary
Aetna considers cardiac CT angiography using less than 64-
intervention; or
slice scanners experimental and investigational because the
o As a technique to evaluate cardiac
effectiveness of this approach has not been established.
function
• Cardiac magnetic resonance imaging
II.
Aetna considers coronary CT angiography experimental
(MRI) is considered investigation and
and investigational for screening of asymptomatic
not medically necessary for the
persons, evaluation of atherosclerotic burden,
following:
evaluation of persons at high pre-test probability of
o Screening for CAD, either in
coronary artery disease, evaluation of stent occlusion
asymptomatic individuals or as
or in-stent restenosis, evaluation of persons with an
part of a preoperative evaluation;
equivocal PET rubidium study, identification
or
of vulnerable plaques, monitoring of atheroma burden,
o Diagnosis of CAD, in individuals
and for all other indications (e.g., atrial
with acute or non-acute
angiosarcoma) because its effectiveness for these
symptoms, or after a coronary
indications has not been established. Note: The
artery intervention.
selection of CT angiography should be made within the
context of other testing modalities such as stress
myocardial perfusion images or cardiac ultrasound
results so that the resulting information facilitates the
management decision and does not merely add a new
layer of testing.
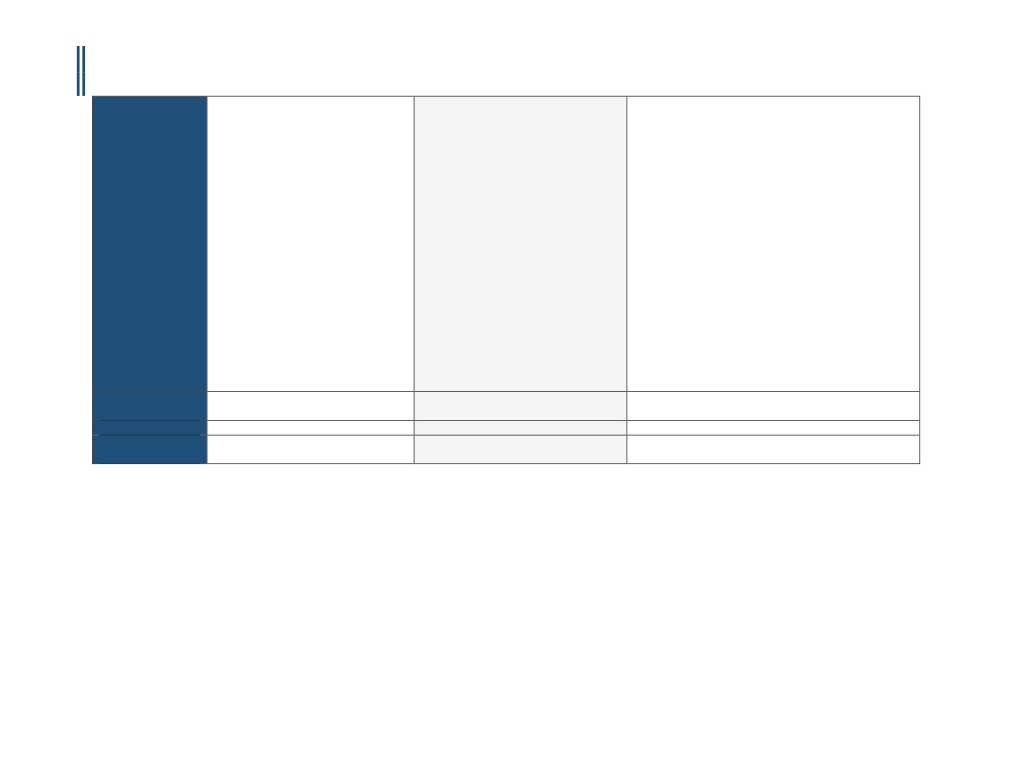
Payer Specific
Requirements
Effective Date
12/28/2016
1/20/2017
Last Review/
11/3/2016
4/9/1998
Original Policy Date
SUGGESTED DOCUMENTATION TO NAVIGATE PRE-AUTHORIZATION
For instances when the indication is medically necessary, clinical evidence is required to determine medical necessity. For instances when the indication is investigational, you
may submit additional information to the Prior Authorization Department. The following documentation is recommended in order to ensure that pre-authorization can be
secured in a timely and efficient manner:
1.
Medical chart notes - all notes from the patient chart related to the requested procedure, including patient’s current cardiac status/ symptoms, cardiac
factors, and indications.
2.
Relevant patient information, including:
▪ Patient age, height, weight, and BMI
▪ Family history of heart problems (including relationship to member, age at diagnosis, type of event, etc.)
▪ Medical history (e.g. diabetes, hypertension, stroke arrhythmia, etc.)
▪ Cardiac risk factors
▪ Previous cardiac treatments, surgeries, or interventions
▪ Problems with exercise capacity
4
CCM-100-131-A

OHIO - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated March 15th, 2017
▪ Ordering provider information
▪ Imaging provider information
▪ Imaging exam(s) being requested (body part, right, left, or bilateral)
▪ Patient diagnosis (suspected or confirmed)
3.
Diagnostic or imaging reports from previous tests (exercise stress test, echocardiography, stress echocardiography, MPI, coronary angiography, etc.)
4.
Symptom history (onset, course, new or changing symptoms) related to all pertinent cardiac conditions, such as heart muscle/ valvular disease, structural
abnormality, infection, exposure to toxins/ chemotherapy, etc.
5.
Examination results, including evaluation of hypertension, heart failure, cardiomyopathy, abnormal rhythm, pulmonary embolus, congenital condition, etc.
6.
Any other documentation that supports the need for the procedure
DISCLAIMER: The information provided in this document is general information only and is not provided as legal advice, nor is it advice about how to code, complete, or submit any particular claim for
payment for health care services or goods. This information provides only an overview of HeartFlow’s understanding of current coverage policies for a select number of payers, and may not provide
all the information necessary to understand a particular patient’s benefits or payers coverage policies and prior authorization requirements. The information provided may not be comprehensive or
complete. It is the responsibility of the health care provider, such as a hospital or a physician to verify coverage and prior authorization requirements, submit complete, accurate and appropriate bills
or claims for payment that comply with applicable laws and regulations and third-party payer requirements, and to determine the appropriate codes, charges, and modifiers that the provider uses for
those purposes. Third-party payers may have policies and coding requirements that differ from those described here, and such policies can change over time.
HeartFlow disclaims any responsibility for claims submitted by health care physicians or others. Physicians should check and verify current policies and requirements with the payer for each patient.
HeartFlow endorses the best practice that all coding and billing submissions to payers be truthful and not misleading, and that providers make full disclosures to the payer about how the service has
been used. HeartFlow cannot guarantee success in obtaining payment for products and services.
Current Procedural Terminology (CPT) copyright 2016.
All rights reserved. CPT® is a registered trademark of the American Medical Association (AMA). Fee schedules, relative value units, conversion factors and/or related components are not assigned by
the AMA, are not part of CPT coding, and the AMA is not recommending their use.
The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) is maintained by the National Center for Health Statistics and the Centers for Medicare and Medicaid
Services.
References:
1.
“Cardiac Checklist (Health Plan).” RadMD, http://www1.radmd.com/media/459739/template-cardiac-checklist-magellan-hc-logo-4-1-2016.pdf. Accessed 25 October 2016.
2.
“ IM Specialty Health ( IM) Ordering Physician/Provider Quick Tips for Diagnostic Imaging Management Programs.” Anthem,
https://www11.anthem.com/provider/nh/f5/s2/t0/pw_ad087257.pdf. Accessed 25 October 2016.
5
CCM-100-131-A