MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
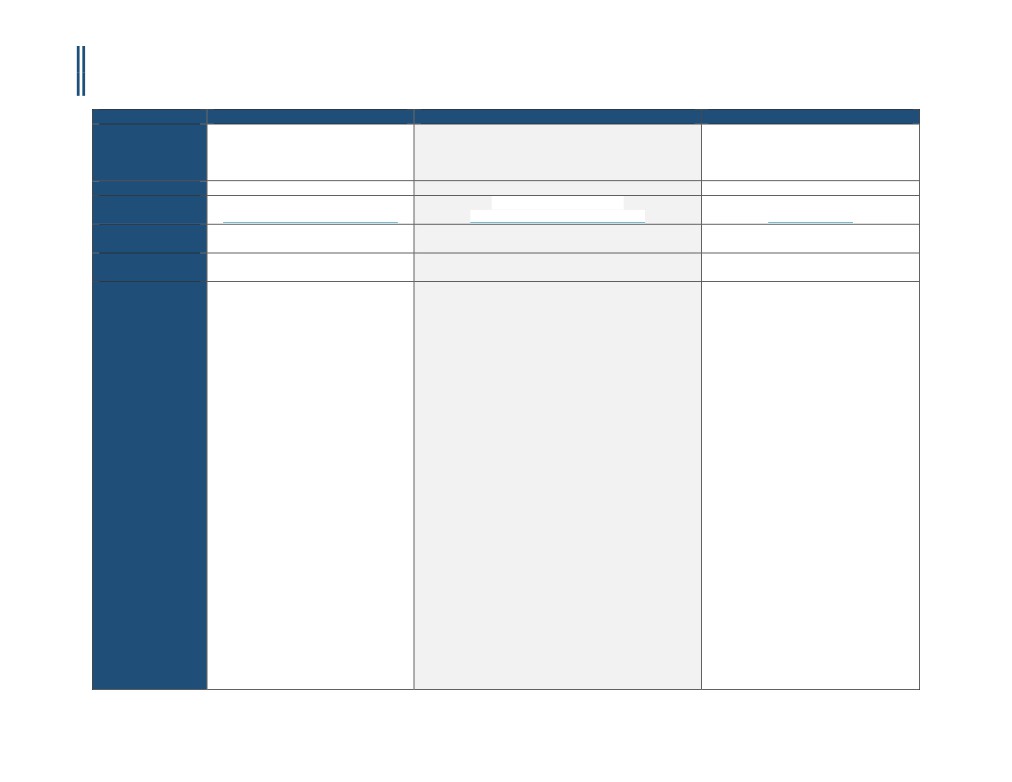
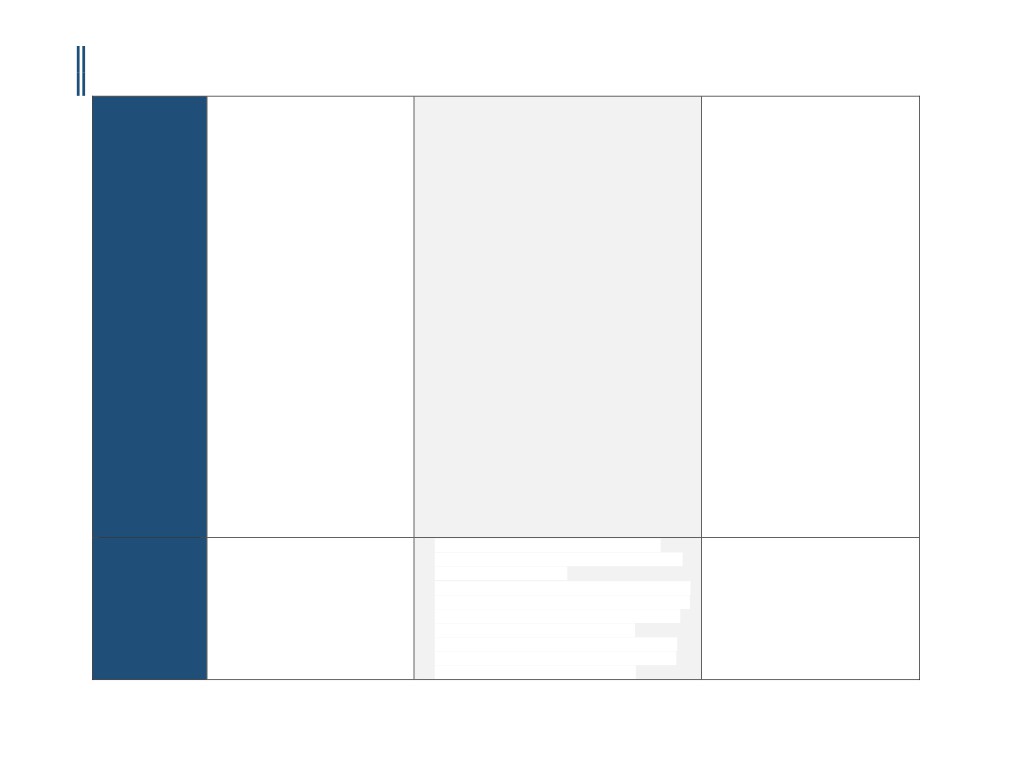
Payer
BlueCross BlueShield Michigan
Priority Health
Health Alliance Plan of Michigan
Policy Name
Clinical Appropriateness Guidelines:
Computerized Tomographic Angiography Coronary
eviCore Cardiac Imaging Guidelines
Advanced Imaging
Arteries (CCTA)
Appropriate Use Criteria: Imaging of the
Heart
Policy #
RAD.00035
91614-R0
CD-8~CT HEART and CCTA
RBM
AIM Specialty Health® (AIM)
AIM Specialty Health® (AIM)
eviCore (Product line and POS dependent)
Applicable CPT
75574
75574, 93799
75574
Code(s)
Applicable ICD
Not Listed
Various - see criteria
Not Listed
Code(s)
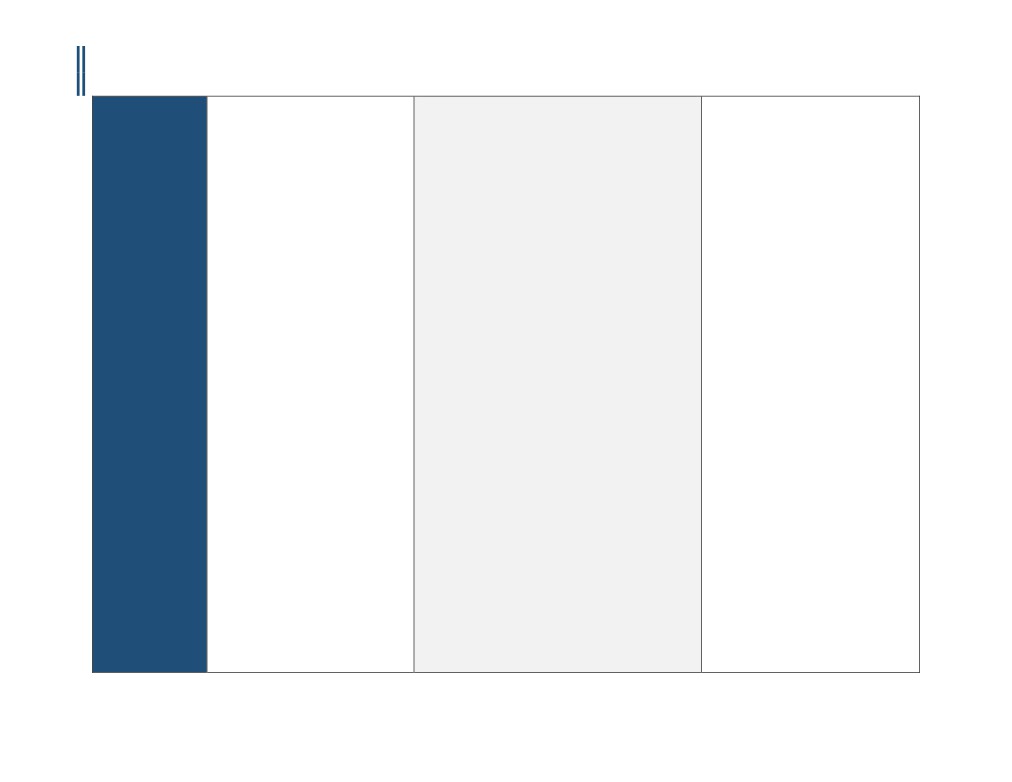
Covered
1.Congenital coronary artery anomalies
The following diagnostic indications for CCTA may be
A. For symptomatic individuals who have a
a. For evaluation of suspected
covered when accompanied by pre-test considerations as
very low, low, or intermediate pretest
congenital anomalies of the
well as supporting clinical data and prerequisite
probability of CAD, CCTA may be used in
coronary arteries
information:
the following situations:
1.Unable to perform either an exercise
2.Congestive Heart Failure/
A. Congenital coronary artery anomalies
or pharmacologic imaging stress test
cardiomyopathy/ left ventricular
1.For evaluation of suspected congenital anomalies of
2.Stress test (treadmill or imaging
dysfunction
the coronary arteries
stress test) is uninterpretable,
a. For exclusion of coronary artery
equivocal, or a false positive is
disease in patients with left
B. Congestive Heart Failure/ cardiomyopathy/ left
suspected
ventricular ejection fraction <55%
ventricular dysfunction
3.Replace performance of invasive
in whom coronary artery disease
1. For exclusion of coronary artery disease in patients
coronary angiogram
has not been excluded as the
with left ventricular ejection fraction <55% and low
B. For symptomatic individuals, evaluate
etiology of the cardiomyopathy
or moderate coronary heart disease risk (using
post-CABG graft patency when only graft
standard methods of risk assessment, such as the
patency is a concern and imaging of the
3.Evaluation of patients with suspected
SCORE risk calculation) in whom coronary artery
native coronary artery anatomy is not
coronary artery disease including those
disease has not been excluded as the etiology of the
needed, such as in early graft failure
with prior abnormal cardiac testing
cardiomyopathy
C. For symptomatic individuals with
(MPI or stress echo)
2. Patients with high coronary heart disease risk
unsuccessful conventional coronary
a. Patients with abnormal MPI or
should undergo cardiac catheterization
angiography
stress echo within the preceding
D. Additional Indications:
60 days suspected to be false
C. Suspected coronary artery disease in asymptomatic
1.Re-do CABG: To identify whether
positive on the basis of low
patients when Fractional Flow Reserve (FFR-CT) can be
bypass grafts are located directly
Coronary Heart Disease Risk (using
calculated in conjunction with imaging
beneath the sternum, so that
standard methods of risk
1. Patients with high-risk of CAD (SCORE) who have
alternative ways to enter the chest
assessment such as the SCORE risk
not had evaluation of coronary artery disease (MPI,
can be planned
calculation)
stress echo, cardiac PET, coronary CTA or cardiac
2.Evaluate coronary artery anomalies
i. In the absence of a
catheterization) within the preceding three (3)
and other complex congenital heart
contraindication (excluding renal
years.
1
CCM-100-117-A
MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
impairment and iodinated
2.Patients with moderate or high risk of CAD (SCORE)
disease of cardiac chambers or great
contrast agent hypersensitivity)
who have a high risk occupation that would
vessels
patients with moderate or high
endanger others in the event of a myocardial
3.Anomalous coronary artery(ies)
Coronary Heart Disease Risk
infarction, (e.g. airline pilot, law-enforcement
suspected for diagnosis or to plan
should be referred for coronary
officer, firefighter, mass transit operator, bus driver)
treatment and less than age 40 with
arteriography; OR
who have not had evaluation of coronary artery
a history that includes one or more of
b.Patients with equivocal MPI or
disease (MPI, stress echo, cardiac PET, coronary CTA
the following
stress echo within the preceding
or cardiac catheterization) within the preceding
i. Persistent exertional chest pain and
60 days who have low or moderate
three (3) years.
normal stress test
Coronary Heart Disease Risk (using
3. Patients with diseases/conditions with which
ii. Full sibling(s) with history of
standard methods of risk
coronary artery disease commonly coexist and who
sudden death syndrome before age
assessment such as the SCORE risk
have not had evaluation of coronary artery disease
30 or with documented anomalous
calculation
(MPI, stress echo, cardiac PET, coronary CTA or
coronary artery
i. In the absence of a
cardiac catheterization) within the preceding three
iii. Resuscitated sudden death and
contraindication (excluding renal
(3) years:
contraindications for conventional
impairment and iodinated
i. Abdominal aortic aneurysm OR
coronary angiography
contrast agent hypersensitivity)
ii. Established and symptomatic peripheral vascular
4.Unexplained new onset of heart
patients with high Coronary
disease OR
failure
Heart Disease Risk should be
iii. Prior history of cerebrovascular accident (CVA),
5.Evaluation of newly diagnosed
referred for coronary
transient ischemia attack (TIA), or carotid
congestive heart failure or
arteriography
endarterectomy (CEA) or high grade carotid
cardiomyopathy
ii. The resulting information from
stenosis (>70%) OR
i. No prior history of coronary artery
the CCTA should facilitate
iv. Chronic renal insufficiency or renal failure
disease, the ejection fraction is less
management decisions and not
4. Patients who have undergone cardiac
than 50 percent, and low or
merely add a new layer of testing
transplantation and have had no evaluation for
intermediate risk on the pre-test
c. Patients at moderate coronary
coronary artery disease within the preceding one (1)
probability assessment AND
heart disease risk (using standard
year.
ii. No exclusions to cardiac CT
methods of risk assessment, such
5. Patients in whom a decision has been made to treat
angiography
as the SCORE risk calculation)
with interleukin 2.
iii. No cardiac catheterization, SPECT,
being evaluated for non-coronary
cardiac PET, or stress
artery cardiac surgery (including
D. Suspected coronary artery disease in symptomatic
echocardiogram has been
valvular and ascending aortic
patients who have not had evaluation of coronary artery
performed since the diagnosis of
surgery) to avoid an invasive
disease (MPI, cardiac PET, stress echo, coronary CTA or
congestive heart failure or
angiogram, where all the necessary
cardiac catheterization) within the preceding sixty (60)
cardiomyopathy
pre-operative information can be
days when Fractional Flow Reserve (FFR-CT) can be
6.Ventricular tachycardia (6 beat runs
obtained using cardiac CT
calculated in conjunction with imaging:
or greater) if CCTA will replace
d.
For evaluation of suspected
1. Chest Pain
conventional invasive coronary
congenital anomalies of the
i. With intermediate or high pretest probability of
angiography
coronary arteries
CAD OR
7.Equivocal coronary artery anatomy
ii. With low or very low pretest probability of CAD
on conventional cardiac
and high risk of CAD (SCORE)
catheterization
2
CCM-100-117-A
MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
2. Atypical symptoms: syncope, shortness of breath
8.Newly diagnosed dilated
(dyspnea), neck, jaw, arm, epigastric or back pain, or
cardiomyopathy
sweating (diaphoresis)
9.Preoperative assessment of the
i. With moderate or high risk of CAD (SCORE)
coronary arteries in patients who are
3. Other symptoms; palpitation, dizziness,
going to undergo surgery for aortic
lightheadedness, near syncope, nausea, vomiting,
dissection, aortic aneurysm, or
anxiety, weakness, fatigue etc.
valvular surgery if CCTA will replace
i. With high risk of CAD (SCORE)
conventional invasive coronary
4.Patients with any cardiac symptom who have
angiography”
diseases/conditions with which coronary artery
10. Vasculitis/Takayasu’s/Kawasaki’s
disease commonly coexists such as:
disease
i. Diabetes mellitus OR
11. Cardiac Trauma: Chest CTA
ii. Abdominal aortic aneurysm OR
(CPT®71275) and CCTA (CPT®75574)
iii. Established and symptomatic peripheral vascular
are useful in detecting aortic and
disease OR
coronary injury and can help in the
iv. Prior history of cerebrovascular accident (CVA),
evaluation of myocardial and
transient ischemia attack (TIA), or carotid
pericardial injury
endarterectomy (CEA) or high grade carotid
stenosis (>70%) OR
v. Chronic renal insufficiency or renal failure
5. Patients who have undergone cardiac
transplantation.
6.Patients in whom a decision has been made to treat
with interleukin 2.
E. Patients with suspected CAD and abnormal exercise
treadmill test (performed without imaging) with low or
moderate coronary heart disease risk (using standard
methods of risk assessment such as the SCORE risk
calculation) when Fractional Flow Reserve (FFR-CT) can
be calculated in conjunction with imaging
1.Abnormal finding on an exercise treadmill test
include chest pain, ST segment change, abnormal BP
response or complex ventricular arrhythmias.
F. Patients with abnormal MPI or stress echo within the
preceding 60 days suspected to be false positive on the
basis of low coronary heart disease risk (using standard
methods of risk assessment such as the SCORE risk
calculation)
1.In the absence of a contraindication (excluding renal
impairment and iodinated contrast agent
3
CCM-100-117-A
MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
hypersensitivity), patients with moderate or high
coronary heart disease risk should be referred for
coronary arteriography
G. Patients with equivocal MPI or stress echo within the
preceding 60 days who have low or moderate coronary
heart disease risk (using standard methods of risk
assessment such as the SCORE risk calculation)
1.In the absence of a contraindication (excluding renal
impairment and iodinated contrast agent
hypersensitivity), patients with high coronary heart
disease risk should be referred for coronary
arteriography
2.The resulting information from the CCTA should
facilitate management decisions and not merely add
a new layer of testing
H. Patients at moderate coronary heart disease risk (using
standard methods of risk assessment, such as the
SCORE risk calculation) being evaluated for non-
coronary artery cardiac surgery (including valvular and
ascending aortic surgery) to avoid an invasive
angiogram, where all the necessary pre-operative
information can be obtained using cardiac CT.
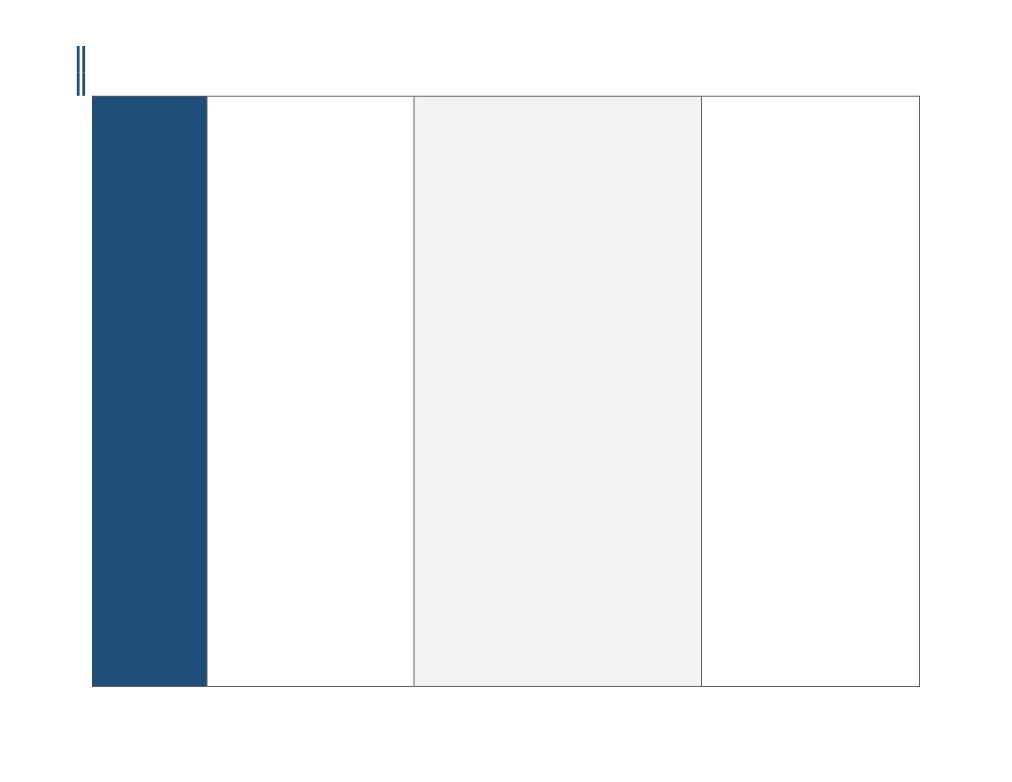
Not Covered /
• Irregular heart rhythms
Investigational and
• Multifocal Atrial Tachycardia (MAT)
Not Medically
• Inability to lie flat
Necessary
• Body mass index of 40 or more
• Inability to obtain a heart rate less than
65 beats per minute after beta-blockers
• Inability to hold breath for at least 8
seconds
• Renal Insufficiency
• Asymptomatic patients and routine use
in the evaluation of the coronary arteries
following heart transplantation
• CCTA should not be performed if there is
extensive coronary calcification (calcium
score >1000)
• Evaluation of coronary stent patency
(metal artifact limits accuracy)
4
CCM-100-117-A
MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
• Evaluation of left ventricular function
following myocardial infarction or in
chronic heart failure
• Evaluation of patients with postoperative
native or prosthetic cardiac valves who
have technically limited
echocardiograms, MRI or TEE. Patients
with indeterminate echocardiogram
should undergo MUGA (CPT®78472 or
CPT®78494) or cardiac MRI
• First test in evaluating symptomatic
patients (e.g. chest pain)
• Irregular heart rhythms
• High pre-test probability for CAD—
rather, these patients should undergo
conventional coronary angiography,
especially if an interventional procedure
(e.g., PCI) is anticipated
• Identification of plaque composition and
morphology
• Myocardial perfusion and viability
studies
• Preoperative assessment for non-
cardiac, nonvascular surgery
• Repeat or routine follow-up of CAD with
CCTA
There is insufficient evidence to support
routine use of Coronary Computed
Tomography Angiography (CCTA) in the
evaluation of the coronary arteries
following heart transplantation.
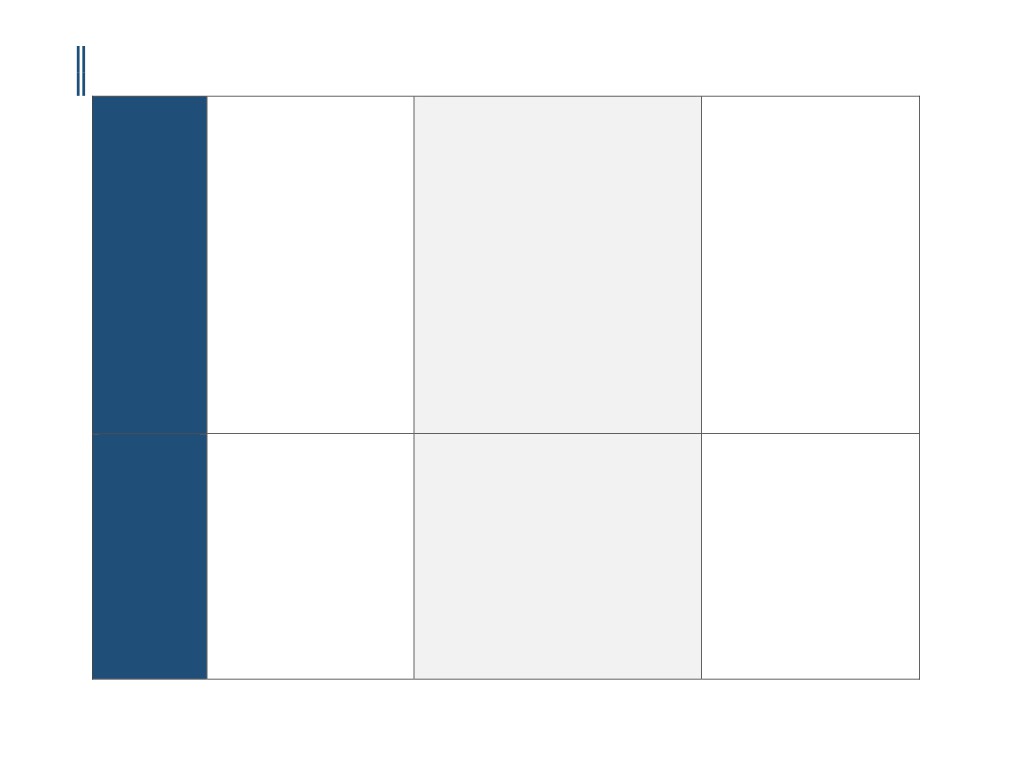
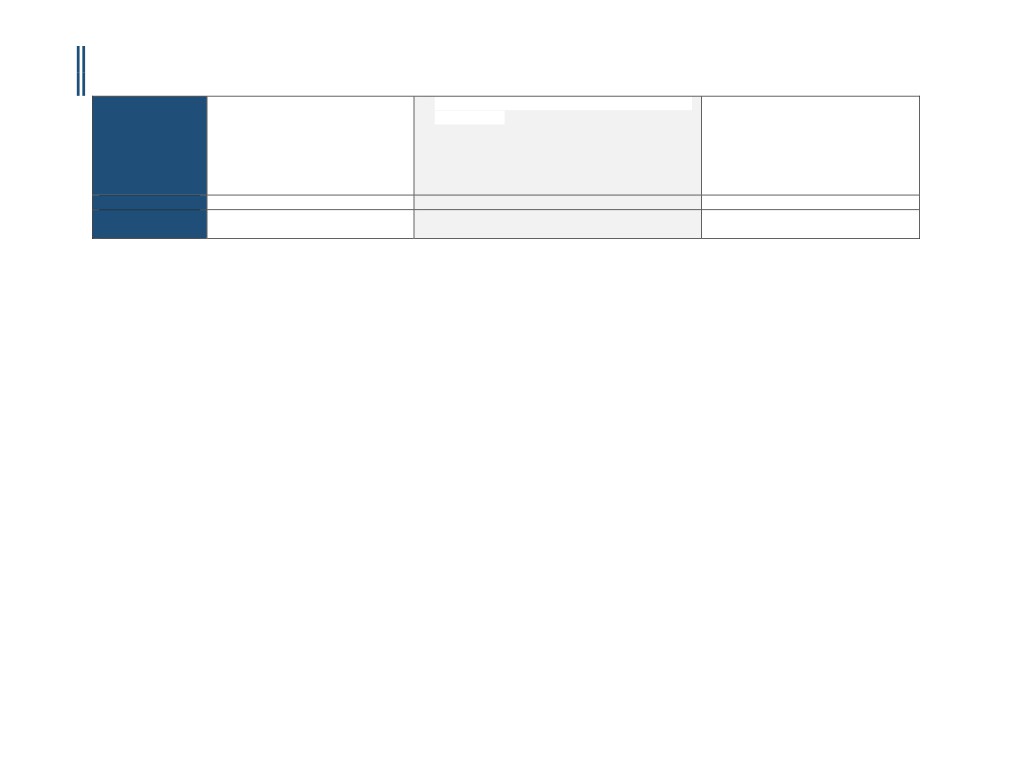
Payer Specific
•
CCTA exams are not covered by most
•
CCTA exams are not covered by most healthcare
1.Must be ordered by a HAP/AHL Affiliated
Requirements
healthcare insurers as a screening
insurers as a screening study, in the absence of signs,
or Contracted Physician
study, in the absence of signs,
symptoms or known disease
2. Must be performed at a HAP/AHL
symptoms or known disease
•
Selection of the optimal diagnostic work-up for cardiac
Affiliated or Contracted Facility.
•
Selection of the optimal diagnostic
evaluation should be made within the context of other
3.Must be authorized be a HAP Medical
work-up for cardiac evaluation should
available studies (which include treadmill stress test,
Director or designee, except for Medicare
be made within the context of other
stress myocardial perfusion imaging, stress
Complementary members with Medicare
available studies (which include
echocardiography, cardiac MRI, cardiac PET imaging
primary and HAP or AHL secondary.
treadmill stress test, stress myocardial
and invasive cardiac/coronary angiography), so that
perfusion imaging, stress
the resulting information facilitates patient
5
CCM-100-117-A
MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
echocardiography, cardiac MRI,
management decisions and does not merely add a new
cardiac PET imaging and invasive
layer of testing
cardiac/coronary angiography), so
that the resulting information
facilitates patient management
decisions and does not merely add a
new layer of testing
Effective Date
10/31/2016
12/1/2015
3/18/2016
Last Review/
7/26/2016
11/11/2015
12/31/2015
Original Policy Date
3/30/2005
SUGGESTED DOCUMENTATION TO NAVIGATE PRE-AUTHORIZATION
For instances when the indication is medically necessary, clinical evidence is required to determine medical necessity. For instances when the indication is investigational, you
may submit additional information to the Prior Authorization Department. The following documentation is recommended in order to ensure that pre-authorization can be
secured in a timely and efficient manner:
1.
Medical chart notes - all notes from the patient chart related to the requested procedure, including patient’s current cardiac status/ symptoms, cardiac
factors, and indications.
2.
Relevant patient information, including:
▪ Patient age, height, weight, and BMI
▪ Family history of heart problems (including relationship to member, age at diagnosis, type of event, etc.)
▪ Medical history (e.g. diabetes, hypertension, stroke arrhythmia, etc.)
▪ Cardiac risk factors
▪ Previous cardiac treatments, surgeries, or interventions
▪ Problems with exercise capacity
▪ Ordering provider information
▪ Imaging provider information
▪ Imaging exam(s) being requested (body part, right, left, or bilateral)
▪ Patient diagnosis (suspected or confirmed)
3.
Diagnostic or imaging reports from previous tests (exercise stress test, echocardiography, stress echocardiography, MPI, coronary angiography, etc.)
4.
Symptom history (onset, course, new or changing symptoms) related to all pertinent cardiac conditions, such as heart muscle/ valvular disease, structural
abnormality, infection, exposure to toxins/ chemotherapy, etc.
5.
Examination results, including evaluation of hypertension, heart failure, cardiomyopathy, abnormal rhythm, pulmonary embolus, congenital condition, etc.
6.
Any other documentation that supports the need for the procedure
DISCLAIMER: The information provided in this document is general information only and is not provided as legal advice, nor is it advice about how to code, complete, or submit any particular claim for
payment for health care services or goods. This information provides only an overview of HeartFlow’s understanding of current coverage policies for a select number of payers, and may not provide
all the information necessary to understand a particular patient’s benefits or payers coverage policies and prior authorization requirements. The information provided may not be comprehensive or
complete. It is the responsibility of the health care provider, such as a hospital or a physician to verify coverage and prior authorization requirements, submit complete, accurate and appropriate bills
or claims for payment that comply with applicable laws and regulations and third-party payer requirements, and to determine the appropriate codes, charges, and modifiers that the provider uses for
those purposes. Third-party payers may have policies and coding requirements that differ from those described here, and such policies can change over time.
6
CCM-100-117-A

MICHIGAN - CORONARY CTA PRIOR-AUTHORIZATION INFORMATIONAL GUIDE
Updated November 18th, 2016
HeartFlow disclaims any responsibility for claims submitted by health care physicians or others. Physicians should check and verify current policies and requirements with the payer for each patient.
HeartFlow endorses the best practice that all coding and billing submissions to payers be truthful and not misleading, and that providers make full disclosures to the payer about how the service has
been used. HeartFlow cannot guarantee success in obtaining payment for products and services.
Current Procedural Terminology (CPT) copyright 2016.
All rights reserved. CPT® is a registered trademark of the American Medical Association (AMA). Fee schedules, relative value units, conversion factors and/or related components are not assigned by
the AMA, are not part of CPT coding, and the AMA is not recommending their use.
The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) is maintained by the National Center for Health Statistics and the Centers for Medicare and Medicaid
Services.
References:
1.
“Cardiac Checklist (Health Plan).” RadMD, http://www1.radmd.com/media/459739/template-cardiac-checklist-magellan-hc-logo-4-1-2016.pdf. Accessed 25 October 2016.
2.
“AIM Specialty Health (AIM) Ordering Physician/Provider Quick Tips for Diagnostic Imaging Management Programs.” Anthem,
https://www11.anthem.com/provider/nh/f5/s2/t0/pw_ad087257.pdf. Accessed 25 October 2016.
7
CCM-100-117-A