JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
VOL.
■, NO. ■, 2017
ª 2017 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
ISSN
0735-1097/≥36.00
PUBLISHED BY ELSEVIER
APPROPRIATE USE CRITERIA
ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/
STS 2017 Appropriate Use Criteria for
Coronary Revascularization in Patients
With Stable Ischemic Heart Disease
A Report of the American College of Cardiology Appropriate Use Criteria Task Force,
American Association for Thoracic Surgery, American Heart Association,
American Society of Echocardiography, American Society of Nuclear Cardiology,
Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography,
and Society of Thoracic Surgeons
Coronary
Manesh R. Patel, MD, FACC, FAHA, FSCAI, Chair
David J. Maron, MD, FACC, FAHA
Revascularization
Peter K. Smith, MD, FACC†
Writing Group
John H. Calhoon, MD
Gregory J. Dehmer, MD, MACC, MSCAI, FAHA*
*Society for Cardiovascular Angiography and Interventions
James Aaron Grantham, MD, FACC
Representative. ySociety of Thoracic Surgeons Representative.
Thomas M. Maddox, MD, MSC, FACC, FAHA
Rating Panel
Michael J. Wolk, MD, MACC, Moderator
Peter L. Duffy, MD, FACC, FSCAI*
Manesh R. Patel, MD, FACC, FAHA, FSCAI,
T. Bruce Ferguson, JR, MD, FACC‡
Writing Group Liaison
Frederick L. Grover, MD, FACC‡
Gregory J. Dehmer, MD, MACC, FSCAI, FAHA,
Robert A. Guyton, MD, FACC‖
Writing Group Liaison*
Mark A. Hlatky, MD, FACC‡
Peter K. Smith, MD, FACC, Writing Group Liaison
Harold L. Lazar, MD, FACC¶
Vera H. Rigolin, MD, FACC‡
James C. Blankenship, MD, MACC, MSCAI‡
Geoffrey A. Rose, MD, FACC, FASE#
Alfred A. Bove, MD, PHD, MACC‡
Richard J. Shemin, MD, FACC‖
Steven M. Bradley, MD§
Jacqueline E. Tamis-Holland, MD, FACC‡
Larry S. Dean, MD, FACC, FSCAI*
Carl L. Tommaso, MD, FACC, FSCAI*
This document was approved by the American College of Cardiology Clinical Policy Approval Committee on behalf of the Board of Trustees in
January 2017.
The American College of Cardiology requests that this document be cited as follows: Patel MR, Calhoon JH, Dehmer GJ, Grantham JA, Maddox TM,
Maron DJ, Smith PK. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 appropriate use criteria for coronary revascularization in patients with stable
ischemic heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery,
American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography
and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J Am Coll Cardiol 2017;69:XXX-XX.
This document has been reprinted in the Journal of Nuclear Cardiology and the Journal of Thoracic and Cardiovascular Surgery.
Copies: This document is available on the World Wide Web site of the American College of Cardiology (www.acc.org ). For copies of this document,
Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the express
permission of the American College of Cardiology. Requests may be completed online via the Elsevier site (http://www.elsevier.com/about/policies/
2
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
L. Samuel Wann, MD, MACC**
‖Society of Thoracic Surgeons Representative. ¶American
Association for Thoracic Surgery Representative. #American Society
John B. Wong, MD‡
of Echocardiography Representative. **American Society of Nuclear
Cardiology Representative.
‡American College of Cardiology Representative.
§American Heart Association Representative.
Appropriate Use
John U. Doherty, MD, FACC, Co-Chair
Warren J. Manning, MD, FACC
Criteria Task
Gregory J. Dehmer, MD, MACC, Co-Chair
Manesh R. Patel, MD, FACC, FAHA§§
Force
Ritu Sachdeva, MBBS, FACC
Steven R. Bailey, MD, FACC, FSCAI, FAHA
L. Samuel Wann, MD, MACC††
Nicole M. Bhave, MD, FACC
David E. Winchester, MD, FACC
Alan S. Brown, MD, FACC††
Michael J. Wolk, MD, MACC††
Stacie L. Daugherty, MD, FACC
Joseph M. Allen, MA
Milind Y. Desai, MBBS, FACC
Claire S. Duvernoy, MD, FACC
††Former Task Force member; current member during the writing
Linda D. Gillam, MD, FACC
effort. ††Former Task Force Co-Chair; current Co-Chair during the
Robert C. Hendel, MD, FACC, FAHA††
writing effort. §§Former Task Force Chair; current Chair during the
Christopher M. Kramer, MD, FACC, FAHA‡‡
writing effort.
Bruce D. Lindsay, MD, FACC††
TABLE OF CONTENTS
ABSTRACT
■
Section 1. SIHD Without Prior CABG
■
Table 1.1 One-Vessel Disease
■
PREFACE
■
Table 1.2 Two-Vessel Disease
■
■
1.INTRODUCTION
■
Table 1.4 Left Main Coronary Artery Stenosis
■
2.METHODS
■
Indication Development
■
Table 2.1 IMA to LAD Patent and Without Significant
Stenoses
■
Figure 1 AUC Development Process
■
Table 2.2 IMA to LAD Not Patent
■
Scope of Indications
■
Which Coronary Revascularization May Be
3.ASSUMPTIONS
■
Considered
■
General Assumptions
■
Table 3.1 Stable Ischemic Heart Disease Undergoing
Procedures for Which Coronary Revascularization
Assumptions for Rating Multiple Treatment Options . . ■
May Be Considered
■
4.DEFINITIONS
■
7.DISCUSSION
■
Table A. Revascularization to Improve Survival
Compared With Medical Therapy
■
APPENDIX A
Table B. Noninvasive Risk Stratification
■
ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS
2017 Appropriate Use Criteria for Coronary
5.ABBREVIATIONS
■
Revascularization in Patients With Stable Ischemic
Heart Disease: Participants
■
6.CORONARY REVASCULARIZATION IN PATIENTS
APPENDIX B
WITH STABLE ISCHEMIC HEART DISEASE:
APPROPRIATE USE CRITERIA (BY INDICATION)
■
Relationships With Industry and Other Entities
■
JACC VOL.
■, NO. ■, 2017
Patel et al.
3
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
ABSTRACT
Interventions, Society of Thoracic Surgeons, American
Association for Thoracic Surgery, and other societies,
The American College of Cardiology, Society for Cardio-
developed and published the first version of the AUC for
vascular Angiography and Interventions, Society of
coronary revascularization in
2009, releasing the last
Thoracic Surgeons, and American Association for Thoracic
update in 2012. The AUC are an effort to assist clinicians
Surgery, along with key specialty and subspecialty soci-
in the rational use of coronary revascularization in
eties, have completed a 2-part revision of the appropriate
common clinical scenarios found in everyday practice.
use criteria (AUC) for coronary revascularization. In prior
The new AUC for coronary revascularization were
coronary revascularization AUC documents, indications for
developed as separate documents for stable ischemic
revascularization in acute coronary syndromes and stable
heart disease (SIHD) and acute coronary syndromes. This
ischemic heart disease (SIHD) were combined into 1 docu-
was done to address the expanding clinical indications
ment. To address the expanding clinical indications for
for coronary revascularization, include new literature
coronary revascularization, and to align the subject matter
published since the last update, and align the subject
with the most current American College of Cardiology/
matter with the ACC/American Heart Association guide-
American Heart Association guidelines, the new AUC for
lines. An additional goal was to address several of the
coronary artery revascularization were separated into 2
shortcomings of the initial document that became
documents addressing SIHD and acute coronary syndromes
evident as experience with the use of the AUC accumu-
individually. This document presents the AUC for SIHD.
lated in clinical practice.
Clinical scenarios were developed to mimic patient pre-
The publication of AUC reflects 1 of several ongoing
sentations encountered in everyday practice. These sce-
efforts by the ACC and its partners to assist clinicians who
narios included information on symptom status; risk level
are caring for patients with cardiovascular diseases and to
as assessed by noninvasive testing; coronary disease
support high-quality cardiovascular care. The ACC/
burden; and, in some scenarios, fractional flow reserve
American Heart Association clinical practice guidelines
testing, presence or absence of diabetes, and SYNTAX score.
provide a foundation for summarizing evidence-based
This update provides a reassessment of clinical scenarios
cardiovascular care and, when evidence is lacking, pro-
that the writing group felt were affected by significant
vide expert consensus opinion that is approved in review
changes in the medical literature or gaps from prior criteria.
by the ACC and American Heart Association. However, in
The methodology used in this update is similar to the initial
many areas, variability remains in the use of cardiovas-
document but employs the recent modifications in the
cular procedures, raising questions of over- or underuse.
methods for developing AUC, most notably, alterations in
The AUC provide a practical standard upon which to
the nomenclature for appropriate use categorization.
assess and better understand variability.
A separate, independent rating panel scored the clin-
We are grateful to the writing committee for the
ical scenarios on a scale of 1 to 9. Scores of 7 to 9 indicate
development of the overall structure of the document and
that revascularization is considered appropriate for the
clinical scenarios and to the rating panel—a professional
clinical scenario presented. Scores of 1 to 3 indicate that
group with a wide range of skills and insights—for their
revascularization is considered rarely appropriate for the
thoughtful deliberation on the merits of coronary revas-
clinical scenario, whereas scores in the mid-range of 4 to 6
cularization for various clinical scenarios. We would also
indicate that coronary revascularization may be appro-
like to thank the parent AUC Task Force and the ACC
priate for the clinical scenario.
staff—Joseph Allen, Leah White, and specifically, Maria
As seen with the prior coronary revascularization AUC,
Velasquez—for their skilled support in the generation of
revascularization in clinical scenarios with high symptom
this document.
burden, high-risk features, and high coronary disease
Manesh R. Patel, MD, FACC, FAHA, FSCAI
burden, as well as in patients receiving antianginal ther-
Chair, Coronary Revascularization Writing Group
apy, are deemed appropriate. Additionally, scenarios
Immediate Past Chair, Appropriate Use Criteria Task Force
assessing the appropriateness of revascularization before
Michael J. Wolk, MD, MACC, Moderator,
kidney transplantation or transcatheter valve therapy are
Appropriate Use Criteria Task Force
now rated. The primary objective of the AUC is to provide
a framework for the assessment of practice patterns that
1. INTRODUCTION
will hopefully improve physician decision making.
In a continuing effort to provide information to patients,
PREFACE
physicians, and policy makers, the Appropriate Use Task
Force approved this revision of the
2012
Coronary
The American College of Cardiology (ACC), in collabora-
Revascularization AUC (1). Since publication of the 2012
tion with the Society for Cardiovascular Angiography and
AUC focused update, the original nomenclature used to
4
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
characterize appropriate use has changed (2). New clinical
encountered in practice, it would be impossible to include
practice guidelines (CPGs) for SIHD have been released,
every conceivable patient presentation and maintain a
and new clinical trials extending the knowledge and evi-
workable document for clinicians. The writing group ac-
dence around coronary revascularization have been pub-
knowledges that the current AUC do not evaluate all pa-
lished (3,4). These trials include studies not only on the
tient variables that might affect 1 or more strategies for
use of percutaneous coronary intervention (PCI), but also
the management of patients with CAD. Examples of con-
on coronary artery bypass graft surgery (CABG), medical
ditions not explicitly considered within the scenarios
therapy, and diagnostic technologies such as fractional
include severe chronic kidney disease, severe peripheral
flow reserve
(FFR) to guide revascularization
(5-8).
vascular disease, known malignancies, poor lung func-
Additional studies, some based on data from the National
tion, advanced liver disease, advanced dementia, and/or
Cardiovascular Data Registry
(NCDR), have been pub-
other comorbidities that might have excluded patients
lished providing insights into practice patterns and in-
from the clinical trials that provide the evidence base for
formation around clinical scenarios and patient features
coronary revascularization. Nevertheless, it is necessary
not previously addressed (9-13).
for the clinician to include these conditions in the final
Improvements in our understanding of the variables
decision-making process for an individual patient, and
affecting patient outcomes before and after coronary
this may result in the actual therapy deviating from the
revascularization, continued emphasis on the role of
AUC rating. It is expected that all clinicians will occa-
medical therapy for coronary artery disease (CAD), and an
sionally treat patients with extenuating conditions that
increasing emphasis on shared decision making and pa-
are not captured in the current AUC, and this could result
tient preferences also make a revision of the coronary
in a treatment rating of “rarely appropriate” for the cho-
revascularization AUC timely (14). This document focuses
sen therapy in a specific patient. However, these situa-
on SIHD and is a companion to the AUC specifically for
tions should not constitute a majority of treatment
acute coronary syndromes.
decisions, and it is presumed that they will affect all
practitioners equally, thereby minimizing substantial
2. METHODS
biases in assessing the performance of individual clini-
cians compared with their peers. Additionally, these AUC
Indication Development
were developed in parallel with efforts to update data
A multidisciplinary writing group consisting of cardio-
collection within the NCDR registries to include data
vascular health outcomes researchers, interventional
fields that capture some of these extenuating circum-
cardiologists, cardiothoracic surgeons, and general car-
stances, thereby improving the characterization of sce-
diologists was convened to review and revise the prior
narios in the AUC.
coronary revascularization AUC. The writing group was
AUC documents often contain specific clinical sce-
tasked with developing clinical indications
(scenarios)
narios rather than the more generalized situations
that reflect typical situations encountered in everyday
covered in CPGs; thus, subtle differences between these
practice that were then rated by a technical panel. In this
documents may exist. The treatment of patients with
document, the term “indication” is used interchangeably
SIHD should always include therapies to modify risk
with the phrase “clinical scenario.” Critical data elements
factors and/or reduce cardiovascular events—so-called
and mapping of the criteria to the elements will be pro-
secondary prevention. In several CPGs, the phrase
vided for end-users of the revascularization AUC so that
“guideline-directed medical therapy” is used and,
procedure notes and chart abstraction can be more easily
depending on the context, may include the use of anti-
mapped to the AUC. A key goal of this effort is to leverage
anginal therapy in addition to therapies for secondary
the NCDR (National Cardiovascular Data Registry) Cath-
prevention. In this AUC, it is assumed that all patients will
PCI registry to map indications to appropriateness ratings,
be receiving comprehensive secondary prevention thera-
so that minimal additional data collection is needed to
pies as needed. Antianginal therapy has a central role in
support quarterly feedback to sites of their performance
the treatment of patients with SIHD. In some patients, it
as a foundation for improving patient selection for
may be the sole therapy, whereas in others it may be
revascularization. The AUC Task Force is committed to
continued, albeit in lower doses, following a revasculari-
supporting linkage of the AUC with daily workflow to
zation procedure. The earlier coronary revascularization
capture the data elements needed for AUC ratings.
AUC included information about the intensity of anti-
The revascularization AUC are based on our current
anginal therapy in several scenarios, with language such
understanding of procedure outcomes plus the potential
as “receiving no or minimal anti-ischemic therapy” or
patient benefits and risks of the revascularization strate-
“receiving a course of maximal anti-ischemic therapy.”
gies examined. Although the AUC are developed to
The new AUC adopts a different format, including options
address many of the common clinical scenarios
for the initiation or escalation of antianginal therapy

JACC VOL.
■, NO. ■, 2017
Patel et al.
5
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
patterned after recommendations made in the 2012 ACCF/
framework to evaluate overall clinical practice patterns
AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diag-
and improve the quality of care.
nosis and Management of Patients With Stable Ischemic
In developing these AUC for coronary revasculariza-
Heart Disease (2012 SIHD guideline) (3), using a structure
tion, the rating panel was asked to rate each indication
that mimics clinical practice. However, the primary pur-
using the following definition of appropriate use:
pose of these AUCs is to rate the appropriateness of
A coronary revascularization is appropriate care
revascularization with the understanding that decisions
when the potential benefits, in terms of survival or
about revascularization are frequently made in the
health outcomes (symptoms, functional status, and/
context of ongoing antianginal therapy. Because recom-
or quality of life), exceed the potential negative
mendations for revascularization or the medical man-
consequences of the treatment strategy.
agement of CAD are found throughout several CPGs, the
AUC ratings herein are meant to unify related CPGs and
The rating panel scored each indication on a scale from
other data sources and provide a useful tool for clinicians.
1 to 9 as follows:
These AUC were developed with the intent of assisting
Score 7 to 9: Appropriate care
patients and clinicians, but they are not intended to
Score 4 to 6: May be appropriate care
diminish the acknowledged complexity or uncertainty of
clinical decision making and should not be used as a
Score 1 to 3: Rarely appropriate care
substitute for sound clinical judgment. There are
Appropriate Use Definition and Ratings
acknowledged evidence gaps in many areas where clinical
judgment and experience must be blended with patient
In rating these criteria, the rating panel was asked to assess
preferences and the existing knowledge base defined in
whether the use of revascularization for each indication is
CPGs. It is important to emphasize that a rating of
“appropriate care,”
“may be appropriate care,” or is
appropriate care does not mandate that a revasculariza-
“rarely appropriate care” using the following definitions
tion procedure be performed; likewise, a rating of rarely
and their associated numeric ranges. Anonymized indi-
appropriate care should not prevent a revascularization
procedure from being performed. It is anticipated, as
Median Score 7 to 9: Appropriate Care
noted in the previous text, that there will be occasional
clinical scenarios rated rarely appropriate in which per-
An appropriate option for management of patients in this
forming revascularization may still be in the best interest
population, as the benefits generally outweigh the risks;
of a particular patient. In situations in which the AUC
an effective option for individual care plans, although not
rating is not followed, clinicians should document the
always necessary depending on physician judgment and
specific patient features not captured in the clinical sce-
patient-specific preferences (i.e., procedure is generally
nario or the rationale for the chosen therapy. Depending
acceptable and is generally reasonable for the indication).
on the urgency of care, convening a heart team or
obtaining a second opinion may be helpful in some of
Median Score 4 to 6: May Be Appropriate Care
these settings.
At times an appropriate option for management of pa-
The AUC can be used in several ways. As a clinical tool,
tients in this population due to variable evidence or
the AUC assist clinicians in evaluating possible therapies
agreement regarding the benefit to risk ratio, potential
under consideration and can help better inform patients
benefit based on practice experience in the absence of
about their therapeutic options. As an administrative and
evidence, and/or variability in the population; effective-
research tool, the AUC provide a means of comparing
ness for individual care must be determined by a patient’s
utilization patterns among providers to thereby derive an
physician in consultation with the patient on the basis of
assessment of an individual clinician’s management
additional clinical variables and judgment along with
strategies compared with his/her peers. It is critical to
patient preferences (i.e., procedure may be acceptable
understand that the AUC should be used to assess an
and may be reasonable for the indication).
overall pattern of clinical care rather than being the final
Median Score 1 to 3: Rarely Appropriate Care
arbitrator of specific individual cases. The ACC and its
collaborators believe that an ongoing review of one’s
Rarely an appropriate option for management of patients
practice using these criteria will help guide more effec-
in this population due to the lack of a clear benefit/risk
tive, efficient, and equitable allocation of healthcare re-
advantage; rarely an effective option for individual care
sources, and ultimately, better patient outcomes.
plans; exceptions should have documentation of the
However, under no circumstances should the AUC be
clinical reasons for proceeding with this care option (i.e.,
used to adjudicate or determine payment for individual
procedure is not generally acceptable and is not generally
patients. Rather, the intent of the AUC is to provide a
reasonable for the indication).
6
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
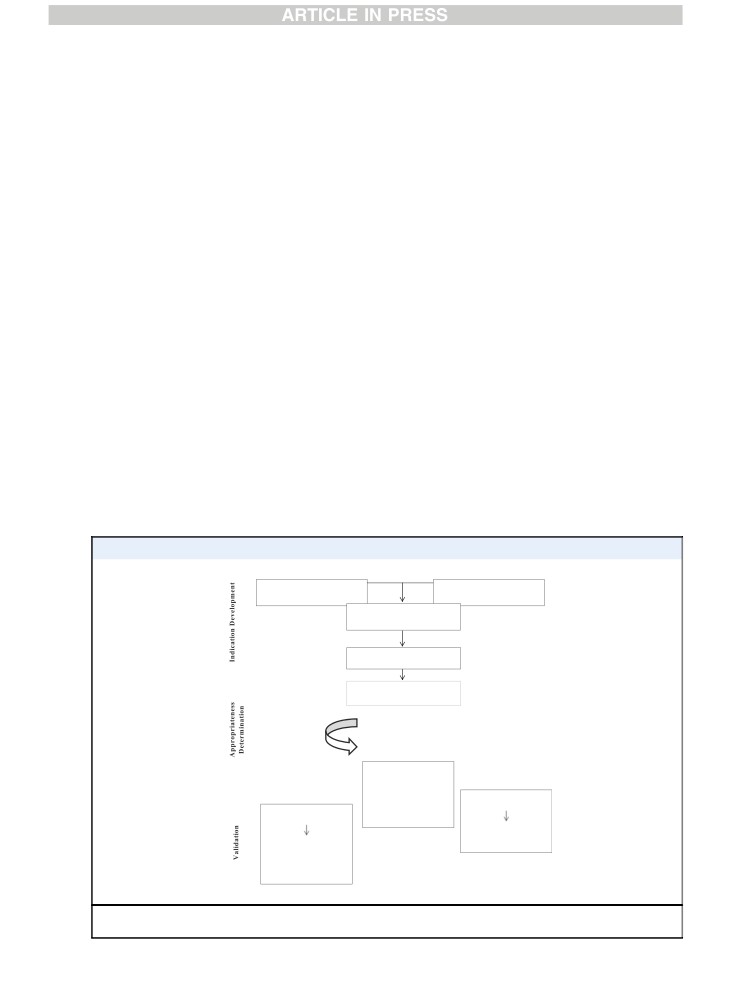
The process for development of the AUC is shown in
7. Invasive testing such as intravascular ultrasound
Figure 1 and described in detail in previous documents
(IVUS) and invasive physiology such as FFR.
(1,2).
The anatomic construct for CAD is based on the pres-
After completion and tabulation of the second round of
ence or absence of flow-limiting obstructions in the cor-
ratings, it became apparent to the writing group that the
onary arteries categorized by the number of vessels
original structure of certain rating tables may have
involved (1-,
2-, and
3-vessel, and/or left main CAD).
confused some members of the rating panel, causing
Additionally, we included in the anatomic construct the
ratings that were not internally consistent. This resulted
presence or absence of proximal left anterior descending
in a re-evaluation and redesign of the rating table struc-
(LAD) disease. This specific stenosis location was identi-
ture, which then required a third round of ratings. This
fied in both the 2011 ACCF/AHA guideline for coronary
AUC document presents the end result of that process and
artery bypass graft surgery (2011 CABG guidelines) and
the results of the third round of ratings.
2012 ACC/AHA/SCAI guideline for percutaneous coronary
intervention (2012 PCI guidelines) and was included in
Scope of Indications
clinical trial recruitment to guide revascularization de-
The indications for coronary revascularization in SIHD were
cisions (6,15,16). Other factors such as diabetes and the
developed considering the following common variables:
complexity of disease were included in certain clinical
1. The clinical presentation
(e.g., low or high activity
scenarios given their effect on cardiac risk and association
level to provoke ischemic symptoms);
with more favorable outcomes from surgical revasculari-
2. Use of antianginal medications;
zation. As before, noninvasive test findings are included
3. Results of noninvasive tests to evaluate the presence
in many scenarios to distinguish patients with a low risk
and severity of myocardial ischemia;
for future adverse events from those with intermediate-
4. Presence of other confounding factors and comorbid-
or high-risk findings, as these terms are routinely used in
ities such as diabetes;
clinical practice.
5. Extent of anatomic disease;
Antianginal treatment of CAD is incorporated into the
6. Prior coronary artery bypass surgery; and
structure of the tables following the pattern of
FIGURE 1
AUC Development Process
Develop list of indications,
Literature review and
assumptions, and definitions
guideline mapping
Review Panel >30 members
provide feedback
Writing Group revises
indications
Rating Panel rates the
indications in 2 rounds
1st round-no interaction
2nd round-panel interaction
Appropriate Use Score
(7-9) Appropriate
(4-6) May Be
Appropriate
Prospective clinical
(1-3) Rarely
decision aids
Prospective comparison
Appropriate
with clinical records
Increase appropriate
use
% use that is
Appropriate, May Be
Appropriate, or Rarely
Appropriate
AUC indicates appropriate use criteria.
JACC VOL.
■, NO. ■, 2017
Patel et al.
7
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
recommendations in the SIHD guideline (see 2012 SIHD
5. A significant coronary stenosis for the purpose of the
guidelines, Section 4.4.3.1.) but without specific drug or
clinical scenarios is defined as:
dose recommendations (3,4). In general, beta blockers are
n
≥70% luminal diameter narrowing, by visual
recommended as the initial treatment for symptom relief
assessment, of an epicardial stenosis measured in
(Class I recommendation), with calcium channel blockers,
the “worst view” angiographic projection;
long-acting nitrates, or ranolazine prescribed in combi-
n
≥50% luminal diameter narrowing, by visual
nation with beta blockers when initial treatment with beta
assessment, of a left main stenosis measured in
blockers is inadequate to control symptoms despite
the “worst view” angiographic projection; or
appropriate dosing. Calcium channel blockers, long-
n
40% to 70% luminal narrowing, by visual assess-
acting nitrates, or ranolazine should be prescribed for
ment, of an epicardial stenosis measured in the
relief of symptoms when beta blockers are contra-
“worst view” angiographic projection with an
indicated or cause unacceptable side effects. Long-acting
abnormal FFR as defined in the following text.
nondihydropyridine calcium channel blockers are
6. An FFR≤0.80 is abnormal and is consistent with
reasonable alternatives to beta blockers as first-line
downstream inducible ischemia.
therapy for antianginal symptoms
(Class IIa, Level of
7. All patients included in these scenarios are receiving
Evidence: B). The use of FFR was incorporated to a greater
needed therapies to modify existing risk factors as
extent than in the previous AUC as more data on the
outlined in CPGs and other documents (17-19). Despite
usefulness of this testing modality have emerged.
the best efforts of the clinician, all patients may not
achieve target goals for cardiac risk factor modifica-
tion. However, a continuing effort and plan of care to
3. ASSUMPTIONS
address risk factors are assumed to exist.
8. For patients with SIHD, the writing group recognizes
General Assumptions
there are many choices for antianginal therapy and
Specific assumptions provided to the rating panel for their
considerable variation in the use and tolerance of
use in rating the relevant clinical scenarios are summa-
antianginal medications among patients. The use of
rized in the following text.
antianginal therapy adopted in this AUC follows the
1.
When available, each clinical scenario includes the
recommendations of the SIHD guideline. Assume that
patient’s clinical status/symptom complex, ischemic
antianginal therapy is prescribed at a dose that
burden as determined by noninvasive functional
adequately controls the patient’s symptoms or is the
testing, burden of coronary atherosclerosis as deter-
maximally tolerated dose for a particular drug.
mined by angiography, and additional invasive
9. Operators performing percutaneous or surgical
testing evaluations by invasive physiology (e.g., FFR,
revascularization have appropriate clinical training
instantaneous wave-free ratio) or intravascular
and experience and have satisfactory outcomes as
imaging.
assessed by quality assurance monitoring (15,20,21).
2. When utilized, stress testing, with or without an
10. Revascularization by either percutaneous or surgical
associated imaging procedure, was performed
methods is performed in a manner consistent with
correctly and with sufficient quality to produce a
established standards of care at centers with quality/
meaningful and accurate result within the limits of
volume standards (15,20,21).
the test performance. Evidence of myocardial viability
11.
In the clinical scenarios, no unusual extenuating cir-
is also an important finding and in some clinical sit-
cumstances exist (e.g., an inability to comply with
uations may influence the decision for revasculariza-
antiplatelet agents, do-not-resuscitate status, a pa-
tion, but it was not used to further expand the number
tient unwilling to consider revascularization, tech-
of indications.
nical reasons rendering revascularization infeasible,
3. As the main focus of this AUC is revascularization,
or comorbidities likely to markedly increase proce-
assume that coronary angiography has been per-
dural risk). If any of these circumstances exist, it is
formed. The rating panel should judge the appropri-
critical that the clinician provide adequate documen-
ateness of revascularization on the basis of the clinical
tation in the medical record to support exclusions
scenario presented, including the coronary disease
from the AUC and the alternative management de-
identified, independent of a judgment about the
cisions made in the patient.
appropriateness of the coronary angiogram in the
12. Patient history and physical examination are assumed
scenario.
to be comprehensive and thorough. Descriptions of
4. Assume no other significant coronary artery stenoses
the patient’s symptoms are assumed to accurately
are present except those specifically described in the
represent the current status of the patient
(e.g.,
clinical scenario.
asymptomatic patients are truly asymptomatic rather
8
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
than asymptomatic due to self-imposed lifestyle
“Appropriate,”
“May Be Appropriate,” or
“Rarely
limitations).
Appropriate” for any given clinical indication.
13. When PCI is being considered in patients with multi-
2. If more than 1 treatment falls into the same appropriate
vessel disease, it may be clinically prudent to perform
use category, it is assumed that patient preference
the procedures in a sequential fashion
(so-called
combined with physician judgment and available local
“staged procedures”). If this is the initial management
expertise will be used to determine the final treatment
plan, the intent for a staged procedure should be
used.
clearly outlined and the appropriateness rating should
apply to the entire revascularization procedure. Spe-
4. DEFINITIONS
cifically, planned staged procedures should not be
assessed by individual arteries but rather in terms of
Definitions of some key terms used throughout the sce-
the plan for the entire revascularization strategy. For
narios are shown in the following text. A complete set of
data collection purposes, this will require document-
definitions is found in Appendix A. These definitions were
ing how the procedure is staged (either PCI or hybrid
provided to and discussed with the rating panel before
revascularization with surgery), and it is assumed that
the rating process started.
all stenoses covered under the umbrella of the plan-
ned staged procedure are functionally significant.
Indication
14. Although the clinical scenarios should be rated on the
A set of patient-specific conditions defines an “indica-
basis of the published literature, the writing committee
tion.” The term “clinical indication” (used interchange-
acknowledges that decisions about coronary artery
ably with “clinical scenario”) provides the context for the
revascularization in patient populations that are poorly
rating of therapeutic options. However, an “appropriate”
represented in the literature are still required in daily
rating assigned by the rating panel does not necessarily
practice. Therefore, rating panel members should as-
mean the therapy is mandatory, nor does a
“rarely
sume that some of the clinical scenarios presented will
appropriate” rating mean it is prohibited.
have low levels of evidence to guide rating decisions.
Risk Factor Modification (Secondary Prevention) and
Key to the application of the AUC in settings where
Antianginal Medical Therapy
there are extenuating circumstances or low levels of
supporting evidence is enhanced documentation by
As previously stated, the indications assume that patients
the clinician to support the clinical decisions made.
are receiving all indicated treatments for the secondary
15. As with all previously published clinical policies, de-
prevention of cardiovascular events. This includes life-
viations by the rating panel from prior published
style and pharmacological interventions according to
documents were directed by new evidence that jus-
guideline-based recommendations. Antianginal medical
tifies such evolution. However, the reader is advised
therapy is incorporated into the structure of the rating
to pay careful attention to the wording of an indica-
tables and should follow the recommendations of the
tion in the present document when making compari-
SIHD guideline, with a beta blocker as initial therapy and
sons to prior publications.
the option to administer calcium channel blockers, long-
16. Indication ratings contained herein supersede the
acting nitrates, and/or ranolazine if the beta blocker is
ratings of similar indications contained in previous
ineffective or not tolerated (3,4).
AUC coronary revascularization documents.
Specific target doses of drugs are not provided as this
must be individualized, but for beta blockers, it is
assumed the dose is sufficient to blunt the exercise heart
Assumptions for Rating Multiple Treatment Options
rate without causing intolerable fatigue, bradycardia, or
1. The goal of this document is to identify revasculariza-
hypotension. It is assumed that the maximally tolerated
tion treatments that are considered reasonable for a
dose of beta blockers is being used before the addition of
given clinical indication. Therefore, each treatment
other drugs, and when other drugs are added, the dose is
option (PCI or CABG) should be rated independently for
titrated to alleviate symptoms or is also the maximally
its level of appropriateness in the specific clinical sce-
tolerated dose. Using multiple drugs at less than optimal
nario, rather than being placed into a forced or artificial
doses is an inefficient and expensive strategy. The SIHD
rank-order comparison against each other. Identifying
guideline recommends calcium channel blockers or long-
options that may or may not be reasonable for specific
acting nitrates if beta blockers are contraindicated or
indications is the goal of this document, rather than
cause unacceptable side effects. The SIHD guideline also
determining a single best treatment for each clinical
recommends adding calcium channel blockers or long-
indication or a rank-order. Therefore, more than
1
acting nitrates to beta blockers for relief of symptoms
treatment or even all treatments may be considered
when initial treatment with beta blockers is unsuccessful.

JACC VOL.
■, NO. ■, 2017
Patel et al.
9
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
Initiating, continuing, or intensifying antianginal therapy
of the LAD proximal to the first major septal and diagonal,
is integrated into the ratings tables along with revascu-
the terms 1-, 2-, and 3-vessel disease do not define the
larization options, as this is typical of real-world practice.
location (i.e., proximal, mid, or distal) of the stenosis in the
artery, which is frequently related to the amount of
Stress Testing and Risk of Findings on Noninvasive Testing
myocardium at risk. Furthermore, the classification of
Stress testing is commonly used for both diagnosis and
diseased vessels does not consider coronary dominance,
risk stratification of patients with CAD. Therapies to
although in practical terms, most consider individuals with
improve survival in patients with SIHD are outlined in
significant disease in the LAD and a left dominant
circumflex to have
3-vessel involvement. Coronary
noninvasive findings associated with high (>3% annual
anomalies are also not considered in this construct.
death or myocardial infarction), intermediate (1% to 3%
Although imperfect, the commonly used classification of
annual death or myocardial infarction) and low
(<1%
1-, 2-, and 3-vessel disease and left main disease remains
annual death or myocardial infarction) risk are outlined in
widely used in clinical practice. Within the context of this
Table B. It is important to note that this table includes
document, the terms 1-, 2-, and 3-vessel disease should be
several noninvasive findings apart from a stress test, such
assumed to mean that each vessel involved (whether the
as resting LV function and a high coronary calcium score
main vessel or a major side branch) provides flow to a
in the assessment of risk. These were not specifically
sufficient amount of myocardium to be clinically impor-
included in the indications of this AUC, but should be
tant. The anatomic definition of 1-, 2-, or 3-vessel disease is
considered as part of the patient profile described in an
now often augmented by the physiological testing of ste-
indication, especially when high and intermediate risk are
nosis significance (e.g., FFR), which can reclassify the he-
used in the indication.
modynamic significance of a stenosis. In the setting of PCI,
when FFR in an artery is >0.80, treatment is deferred and
Vessel Disease
the clinical scenario considered should be reclassified to be
The construct used to characterize the extent of CAD is
consistent with the number of significant stenoses. In
based on the common clinical use of the terms 1-, 2-, and 3-
other words, if the angiogram suggests 2 significant ste-
vessel disease and left main disease, although it is recog-
noses, but FFR testing indicates that only 1 is significant,
nized that individual coronary anatomy is highly variable.
the clinical scenario considered should be from the group
In general, these terms refer to a significant stenosis in 1 of
with 1-vessel CAD. Although there are considerable data to
the 3 major coronary arteries (right coronary artery, LAD, or
support FFR-directed PCI treatment as an option, this
circumflex) or their major branches. With the exception of
concept is not well-established for surgical revasculariza-
the proximal LAD, which specifically refers to the segment
tion (22,23).
TABLE A Revascularization to Improve Survival Compared With Medical Therapy
Anatomic
Setting
COR
LOE
References
UPLM or complex CAD
CABG and PCI I—Heart Team approach recommended
C
(950-952)
CABG and PCI IIa—Calculation of STS and SYNTAX scores
B
(949,950,953-957)
UPLM*
CABG
I
B
(73,381,412,959-962)
PCI
IIa—For SIHD when both of the following are present:
B
(949,953,955,958,963-980)
■ Anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of
good long-term outcome (e.g., a low SYNTAX score of #22, ostial or trunk left main CAD)
■ Clinical characteristics that predict a significantly increased risk of adverse surgical outcomes
(e.g., STS-predicted risk of operative mortality ≥5%)
IIa—For UA/NSTEMI if not a CABG candidate
B
(949,968-971,976-979,981)
IIa—For STEMI when distal coronary flow is TIMI flow grade <3 and PCI can be performed more
C
(965,982,983)
rapidly and safely than CABG
IIb—For SIHD when both of the following are present:
B
(949,953,955,958,963-980,984)
■ Anatomic conditions associated with a low to intermediate risk of PCI procedural complications
and an intermediate to high likelihood of good long-term outcome (e.g., low-intermediate
SYNTAX score of <33, bifurcation left main CAD)
■ Clinical characteristics that predict an increased risk of adverse surgical outcomes
(e.g., moderate—severe COPD, disability from prior stroke, or prior cardiac surgery;
STS-predicted operative mortality >2%)
III: Harm—For SIHD in patients (versus performing CABG) with unfavorable anatomy for PCI and who are
B
(73,381,412,949,953,955,959-964)
good candidates for CABG
Continued on the next page
10
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
TABLE A Continued
Anatomic
Setting
COR
LOE
References
3-vessel disease with or without proximal LAD artery disease*
CABG
I
B
(353,412,959,985-987)
IIa—It is reasonable to choose CABG over PCI in patients with complex 3-vessel CAD
B
(964,980,987-989)
(e.g., SYNTAX score >22) who are good candidates for CABG.
PCI
IIb—Of uncertain benefit
B
(366,959,980,985,987)
2-vessel disease with proximal LAD artery disease*
CABG
I
B
(353,412,959,985-987)
PCI
IIb—Of uncertain benefit
B
(366,959,985,987)
2-vessel disease without proximal LAD artery disease*
CABG
IIa—With extensive ischemia
B
(327,990-992)
IIb—Of uncertain benefit without extensive ischemia
C
(987)
PCI
IIb—Of uncertain benefit
B
(366,959,985,987)
1-vessel proximal LAD artery disease
CABG
IIa—With LIMA for long-term benefit
B
(412 987,993,994)
PCI
IIb—Of uncertain benefit
B
(366,959,985,987)
1-vessel disease without proximal LAD artery involvement
CABG
III: Harm
B
(306,327,412,985,990,995-998)
PCI
III: Harm
B
(306,327,412,985,990,995-998)
LV dysfunction
CABG
IIa—EF 35% to 50%
B
(365,412,999-1002)
CABG
IIb—EF <35% without significant left main CAD
B
(355,365,410,412,999-1002)
PCI
Insufficient data
N/A
Survivors of sudden cardiac death with presumed ischemia-mediated VT
CABG
I
B
(350,1003,1004)
PCI
I
C
(1003)
No anatomic or physiological criteria for revascularization
CABG
III: Harm
B
(306,327,412,985,990,995-998)
PCI
III: Harm
B
(306,327,412,985,990,995-998)
*In patients with multivessel disease who also have diabetes mellitus, it is reasonable to choose CABG (with LIMA) over PCI (30,991,1005-1011) (Class IIa; LOE: B).
Reproduced from Fihn et al. (3).
CABG indicates coronary artery bypass graft; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; COR, class of recommendation; EF, ejection fraction; LAD, left anterior
descending; LIMA, left internal mammary artery; LOE, level of evidence; LV, left ventricular; N/A, not available; PCI, percutaneous coronary intervention; SIHD, stable ischemic heart disease;
STEMI, ST-elevation myocardial infarction; STS, Society of Thoracic Surgeons; SYNTAX, Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery; TIMI, Thrombolysis
In Myocardial Infarction; UA/NSTEMI, unstable angina/non-ST-elevation myocardial infarction; UPLM, unprotected left main disease; and VT, ventricular tachycardia.
JACC VOL.
■, NO. ■, 2017
Patel et al.
11
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
TABLE B Noninvasive Risk Stratification
High risk (>3% annual death or MI)
1. Severe resting LV dysfunction (LVEF <35%) not readily explained by noncoronary causes
2. Resting perfusion abnormalities ≥10% of the myocardium in patients without prior history or evidence of MI
3. Stress ECG findings including ≥2 mm of ST-segment depression at low workload or persisting into recovery, exercise-induced ST-segment elevation, or
exercise-induced VT/VF
4. Severe stress-induced LV dysfunction (peak exercise LVEF <45% or drop in LVEF with stress ≥10%)
5. Stress-induced perfusion abnormalities encumbering ≥10% myocardium or stress segmental scores indicating multiple vascular territories with
abnormalities
6. Stress-induced LV dilation
7. Inducible wall motion abnormality (involving >2 segments or 2 coronary beds)
8. Wall motion abnormality developing at low dose of dobutamine (#10 mg/kg/min) or at a low heart rate (<120 beats/min)
9. CAC score >400 Agatston units
10. Multivessel obstructive CAD (≥70% stenosis) or left main stenosis (≥50% stenosis) on CCTA
Intermediate risk (1% to 3% annual death or MI)
1. Mild/moderate resting LV dysfunction (LVEF 35% to 49%) not readily explained by noncoronary causes
2. Resting perfusion abnormalities in 5% to 9.9% of the myocardium in patients without a history or prior evidence of MI
3. ≥1 mm of ST-segment depression occurring with exertional symptoms
4. Stress-induced perfusion abnormalities encumbering 5% to 9.9% of the myocardium or stress segmental scores (in multiple segments) indicating 1 vascular
territory with abnormalities but without LV dilation
5. Small wall motion abnormality involving 1 to 2 segments and only 1 coronary bed
6. CAC score 100 to 399 Agatston units
7. One vessel CAD with ≥70% stenosis or moderate CAD stenosis (50% to 69% stenosis) in ≥2 arteries on CCTA
Low risk (<1% annual death or MI)
1. Low-risk treadmill score (score ≥5) or no new ST segment changes or exercise-induced chest pain symptoms; when achieving maximal levels of exercise
2. Normal or small myocardial perfusion defect at rest or with stress encumbering <5% of the myocardium*
3. Normal stress or no change of limited resting wall motion abnormalities during stress
4. CAC score <100 Agaston units
5. No coronary stenosis >50% on CCTA
*Although the published data are limited; patients with these findings will probably not be at low risk in the presence of either a high-risk treadmill score or severe resting LV
dysfunction (LVEF <35%).
Reproduced from Fihn et al. (3).
CAC indicates coronary artery calcium; CAD, coronary artery disease; CCTA, coronary computed tomography angiography; LV, left ventricular; LVEF, left ventricular ejection fraction;
and MI, myocardial infarction.
Ischemic Symptoms
variability in the assessment of symptom severity, the
Angina pectoris is usually described as a discomfort (not
writing group chose not to use the Canadian Cardiovascular
necessarily pain) in the chest or adjacent areas. It is
Society classification system in this document
(24,25).
variably described as tightness, heaviness, pressure,
Symptom status of the patient was broadly classified into
squeezing, or a smothering sensation. In some patients,
asymptomatic or simply ischemic symptoms, emphasizing
the symptom may be a more vague discomfort, a
the use of more objective measures of ischemia within each
numbness, or a burning sensation. Alternatively, so-
indication to stratify patients into low-risk or intermediate-/
called anginal equivalents such as dyspnea, faintness,
high-risk findings.
or fatigue may occur. The location is usually substernal
Invasive Methods of Determining Hemodynamic Significance
and radiation may occur to the neck, jaw, arms, back, or
epigastrium. Isolated epigastric discomfort or pain in the
The writing group recognizes that not all patients referred
lower mandible may rarely be a symptom of myocardial
for revascularization will have previous noninvasive
ischemia. The typical episode of angina pectoris begins
testing. In fact, there are several situations in which pa-
gradually and reaches its maximum intensity over a
tients may be appropriately referred for coronary angi-
period of minutes. Typical angina pectoris is precipi-
ography on the basis of symptom and ECG presentation
tated by exertion or emotional stress and is relieved
and a high pretest probability of CAD. In these settings,
within minutes by rest or nitroglycerin. Because of the
there may be situations where angiography shows a cor-
variation in symptoms that may represent myocardial
onary narrowing of questionable hemodynamic impor-
ischemia, the clinical scenarios are presented using the
tance in a patient with symptoms that can be related to
broad term
“ischemic symptoms” to capture this
myocardial ischemia. In such patients, the use of addi-
concept.
tional invasive measurements (such as FFR or intravas-
This AUC document is specific for patients with SIHD.
cular ultrasound) at the time of diagnostic angiography
Therefore, by definition, there are no Canadian Cardiovas-
may be very helpful in further defining the need for
cular Society Class 4 patients. Because of the variety of
revascularization and may substitute for stress test find-
symptoms that may indicate myocardial ischemia, individual
ings. Accordingly, many of the indications now include
patient variation in how they are described and observer
FFR test results.

12
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
The Role of Patient Preference in the AUC
BB = beta-blockers
Patients often make decisions about medical treatments
CABG = coronary artery bypass graft
without a complete understanding of their options. Pa-
CAD = coronary artery disease
tient participation or shared decision making (SDM) de-
FFR = fractional flow reserve
scribes a collaborative approach whereby patients are
IMA = internal mammary artery
provided with evidence-based information on treatment
choices and encouraged to use the information in an
LAD = left anterior descending coronary artery
informed dialogue with their provider to make decisions
LVEF = left ventricular ejection fraction
that not only use the scientific evidence, but also align
PCI = percutaneous coronary intervention
with their values, preferences, and lifestyle (26-28). The
SIHD = stable ischemic heart disease
alternative decision paradigm, often referred to as medi-
cal paternalism, places decision authority with physicians
and assigns the patient a more passive role (29). SDM re-
6. CORONARY REVASCULARIZATION IN
spects both the provider’s knowledge and the patient’s
PATIENTS WITH STABLE ISCHEMIC HEART
right to be fully informed of all care options with their
DISEASE: APPROPRIATE USE CRITERIA (BY
associated risks and benefits. SDM often uses decision
INDICATION)
aids such as written materials, online modules, or videos
to present information about treatment options that help
Section 1. SIHD Without Prior CABG
the patient evaluate the risks and benefits of a particular
treatment. The most effective decision aids to help pa-
The format for tables in Section 1 is similar, with separate
tients make truly informed decisions provide relevant
tables for 1-, 2-, and 3-vessel disease and left main dis-
facts and videos of real patient perspectives regarding the
ease. The columns in each table are stratified into 2 cat-
particular treatment
(30). Many professional organiza-
egories. There is a single column combining patients who
tions now endorse SDM in practice (31,32).
are asymptomatic and not receiving antianginal therapy
More than 1 treatment option often exists with no clear
with patients who are asymptomatic and receiving anti-
evidence identifying the best option. This is compounded
anginal therapy. The remaining columns are devoted to
when there is variation in experts’ recommendations
patients with ischemic symptoms, with 3 separate cate-
about the best treatment under different circumstances
gories: ischemic symptoms and receiving no antianginal
therapy, ischemic symptoms and receiving 1 antianginal
(33). A challenging situation exists when scientific data
drug (beta blocker preferred), and ischemic symptoms
suggest 1 treatment is likely to have better outcomes, yet
receiving 2 or more antianginal drugs. As outlined in the
the patient prefers an alternative treatment. Within the
SIHD guideline, in the absence of contraindications,
context of the AUC, this would be manifest as the patient
initial therapy should be a beta blocker prescribed at a
requesting a therapy with a lower AUC rating
(e.g.,
dose that reduces heart rate without excessive resting
wanting a therapy rated as rarely appropriate when a
bradycardia, hypotension, or fatigue. Other antianginal
therapy rated appropriate exists). Informed consent is
drugs are then added to beta blockers depending on the
fundamental to SDM (34). Without understanding the pros
individual needs of the patient until symptoms are sup-
and cons of all treatment options, patients cannot properly
pressed to the satisfaction of the patient or higher doses
engage in SDM and blend their personal desires with the
cannot be used because of side effects. In each of the
scientific data. Without question, it is important that
subordinate columns, the panel was asked to rate the
blending AUC ratings into clinical decision making provide
options for revascularization, specifically PCI or CABG. As
a pathway for including patient preference and SDM.
However, the mechanism for that process is beyond the
noted earlier, the rating panel was asked to rate each
scope of this AUC document. The purpose of this docu-
revascularization option independent of the other, with
ment is to develop clinical scenarios and provide ratings of
the intent to rate each therapy on its own merits rather
those scenarios by an expert panel. A complete discussion
than in comparison to the other option. In this construct,
about treatment options with SDM can only be finalized
both revascularization options could be assigned identical
once the category of appropriate use is determined.
ratings.
In this and subsequent tables, clinical scenarios often
contain the phrase “noninvasive testing.” In this docu-
5. ABBREVIATIONS
ment, that phrase includes all forms of stress testing using
either dynamic or pharmacological stress that may be
AA = antianginal
coupled with various imaging tests. It also could include
ACS = acute coronary syndrome
other imaging, such as coronary computed tomography
AUC = appropriate use criteria
angiography or magnetic resonance imaging, to assess

JACC VOL.
■, NO. ■, 2017
Patel et al.
13
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
myocardial viability. Some would favor the term “func-
the equivalent of 2-vessel disease (i.e., right coronary
tional testing,” but the writing committee did not view
artery and circumflex disease). Following this construct,
this as inclusive of computed tomography or magnetic
the combination of proximal LAD disease and proximal
resonance imaging and thus favored the term “noninva-
left dominant circumflex disease would be considered as
sive testing.” FFR is considered as part of an invasive
3-vessel disease and rated using the 3-vessel disease table
evaluation and is cited separately in some scenarios. An
(
Table
1.3.
). In the absence of exercise data, invasive
emerging technology, computed tomography-derived
physiological testing of both involved vessels is included
FFR is a combination technique that is noninvasive like
in several of the indications. To remain in this table of
computed tomography but provides FFR, which has
2-vessel disease, such testing must be abnormal in both
traditionally only been an invasive test.
vessels. If this testing shows only 1 vessel to be abnormal,
the patient would no longer be rated using this table, but
Table 1.1. One-Vessel Disease
rather would be rated in the table for
1-vessel CAD.
Similar to the 2011 CABG and 2012 SIHD guidelines, this
Finally, because of the increasing body of literature that
document uses proximal LAD disease as an additional
has identified diabetes as an important factor to consider
anatomic discriminator for 1-vessel CAD. Although data
when recommending revascularization, scenarios indi-
are minimal, the writing committee felt that proximal
cating the presence of diabetes are provided.
disease of a dominant circumflex should be considered as
high-risk anatomy with similar implications as proximal
Table 1.3
. Three-Vessel Disease
LAD disease, and thus, it was considered in a separate
Similar to Table 1.2, because of the increasing body of
section along with proximal LAD disease.
literature that has identified diabetes as an important
factor to consider when recommending revascularization,
Table 1.2 Two-Vessel Disease
categories indicating the presence or absence of diabetes
The format of this table is similar to that for 1-vessel
are provided among the individual indications. Stenosis
disease. Similar to the 2011 CABG and 2012 SIHD guide-
complexity is also an important factor to consider in any
lines, this document makes a distinction regarding the
revascularization procedure, probably more so for PCI
presence or absence of proximal LAD disease. The writing
than for CABG. The SYNTAX (Synergy between Percuta-
group did not add proximal left dominant circumflex
neous Coronary Intervention with TAXUS and Cardiac
disease as an additional discriminator, because most
Surgery) trial provided a comprehensive comparison of
would consider an isolated stenosis in this location to be
PCI and CABG and a structure that may be helpful in
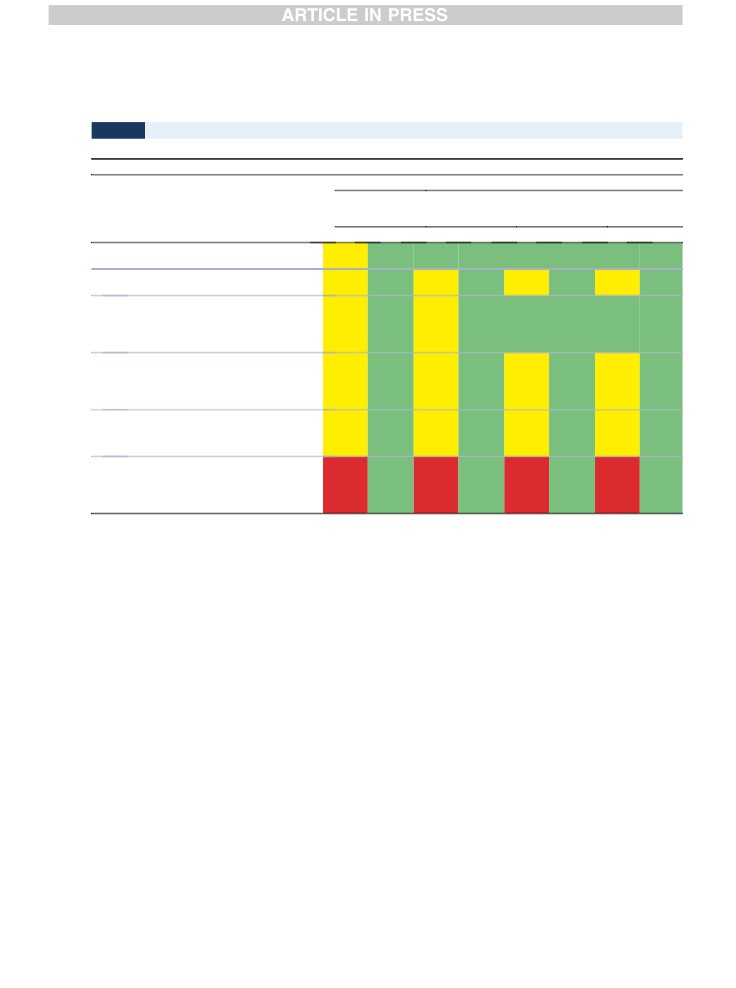
TABLE 1.1
One-Vessel Disease
Appropriate Use Score (1-9)
One-Vessel Disease
Asymptomatic
Ischemic Symptoms
Not on AA
Therapy or With
Not on AA
On 1 AA Drug
AA Therapy
Therapy
(BB Preferred)
On ≥2 AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
No Proximal LAD or Proximal Left Dominant LCX Involvement
1.
■ Low-risk findings on noninvasive testing
R (2)
R (1)
R (3)
R (2)
M (4)
R (3)
A (7)
M (5)
2.
■ Intermediate- or high-risk findings on
M (4)
R (3)
M (5)
M (4)
M (6)
M (4)
A (8)
M (6)
noninvasive testing
3.
■ No stress test performed or, if performed,
M (4)
R (2)
M (5)
R (3)
M (6)
M (4)
A (8)
M (6)
results are indeterminate
■ FFR #0.80*
Proximal LAD or Proximal Left Dominant LCX Involvement Present
4.
■ Low-risk findings on noninvasive testing
M (4)
R (3)
M (4)
M (4)
M (5)
M (5)
A (7)
A (7)
5.
■ Intermediate- or high-risk findings on
M (5)
M (5)
M (6)
M (6)
A (7)
A (7)
A (8)
A (8)
noninvasive testing
6.
■ No stress test performed or, if performed,
M (5)
M (5)
M (6)
M (6)
M (6)
M (6)
A (8)
A (7)
results are indeterminate
■ FFR #0.80
The number in parentheses next to the rating reflects the median score for that indication. *iFR measurements with appropriate normal ranges may be substituted for FFR.
A indicates appropriate; AA, antianginal; BB, beta blockers; CABG, coronary artery bypass graft; FFR, fractional flow reserve; iFR, instant wave-free ratio; LAD, left anterior descending coronary
artery; LCX, left circumflex artery; M, may be appropriate; PCI, percutaneous coronary intervention; and R, rarely appropriate.

14
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
TABLE 1.2
Two-Vessel Disease
Appropriate Use Score (1-9)
Two-Vessel Disease
Asymptomatic
Ischemic Symptoms
Not on AA
Therapy or With
Not on AA
On 1 AA Drug
AA Therapy
Therapy
(BB Preferred)
On ≥2
AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
No Proximal LAD Involvement
7.
■ Low-risk findings on noninvasive testing
R (3)
R (2)
M (4)
R (3)
M (5)
M (4)
A (7)
M (6)
8.
■ Intermediate- or high-risk findings on
M (5)
M (4)
M (6)
M (5)
A (7)
M (6)
A (8)
A (7)
noninvasive testing
9.
■ No stress test performed or, if performed,
M (5)
M (4)
M (6)
M (4)
A (7)
M (5)
A (8)
A (7)
results are indeterminate
■ FFR #0.80* in both vessels
Proximal LAD Involvement and No Diabetes Present
10.
■ Low-risk findings on noninvasive testing
M (4)
M (4)
M (5)
M (5)
M (6)
M (6)
A (7)
A (7)
11.
■ Intermediate- or high-risk findings on
M (6)
M (6)
A (7)
A (7)
A (7)
A (7)
A (8)
A (8)
noninvasive testing
12.
■ No stress test performed or, if performed,
M (6)
M (6)
M (6)
M (6)
A (7)
A (7)
A (8)
A (8)
results are indeterminate
■ FFR #0.80 in both vessels
Proximal LAD Involvement With Diabetes Present
13.
■ Low-risk findings on noninvasive testing
M (4)
M (5)
M (4)
M (6)
M (6)
A (7)
A (7)
A (8)
14.
■ Intermediate- or high-risk findings on
M (5)
A (7)
M (6)
A (7)
A (7)
A (8)
A (8)
A (9)
noninvasive testing
15.
■ No stress test performed or, if performed,
M (5)
M (6)
M (6)
A (7)
A (7)
A (8)
A (7)
A (8)
results are indeterminate
■ FFR #0.80 in both vessels*
The number in parentheses next to the rating reflects the median score for that indication. *iFR measurements with appropriate normal ranges may be substituted for FFR.
A indicates appropriate; AA, antianginal; BB, beta blockers; CABG, coronary artery bypass graft; FFR, fractional flow reserve; iFR, instant wave-free ratio; LAD, left anterior descending coronary
artery; M, may be appropriate; PCI, percutaneous coronary intervention; and R, rarely appropriate.
formulating revascularization recommendations
(35).
procedures and, more recently, comparisons with PCI in
Factors such as vessel occlusion, bifurcation or trifurca-
some anatomic situations. There are data suggesting that
tion at branch points, ostial stenosis location, length
stenting of the left main ostium or trunk is more
>20 mm, tortuosity, calcification, and thrombus all add to
straightforward than treating distal bifurcation or trifur-
the complexity of PCI. The presence of multiple complex
cation stenoses and is associated with a lower rate of
features
(SYNTAX score >22) is associated with more
restenosis. In comparison, left main lesion location has a
favorable outcomes with CABG. Although limitations of
negligible influence on the success and long-term results
the SYNTAX score for certain revascularization recom-
of CABG. Accordingly, there are separate rating options
mendations are recognized and it may be impractical to
for ostial and mid-shaft left main disease and distal or
apply this scoring system to all patients with multivessel
bifurcation left main disease. The definition of a signifi-
disease, it is a reasonable surrogate for the extent and
cant left main stenosis used herein is ≥50% narrowing by
complexity of CAD and provides important information
angiography. However, the angiographic assessment of
that can be helpful when making revascularization
the severity of left main disease has several shortcomings,
decisions.
and other assessments such as IVUS or FFR may be
Accordingly, in this table specifically for patients with
needed. For left main coronary artery stenoses, a mini-
3-vessel disease, the rating panel was asked to consider
mum lumen diameter of <2.8 mm or a minimum lumen
the indications in patients with low complexity compared
area of
<6 mm2 suggests a physiologically significant
with those with intermediate and high complexity.
lesion. It has been suggested that a minimum lumen area
>7.5 mm2 suggests revascularization may be safely de-
Table 1.4. Left Main Coronary Artery Stenosis
ferred. A minimum lumen area between 6 and 7.5 mm2
Literature on the treatment of significant left main dis-
requires further physiological assessment, such as mea-
ease is dominated by surgical revascularization
surement of FFR. Alternatively, FFR may be used as the

JACC VOL.
■, NO. ■, 2017
Patel et al.
15
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
TABLE 1.3
Three-Vessel Disease
Appropriate Use Score (1-9)
Three-Vessel Disease
Asymptomatic
Ischemic Symptoms
Not on AA
Therapy or With
Not on AA
On 1 AA Drug
AA Therapy
Therapy
(BB Preferred)
On ≥2
AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
Low Disease Complexity (e.g., Focal Stenoses, SYNTAX #22)
16.
■ Low-risk findings on noninvasive testing
M (4)
M (5)
M (5)
M (5)
M (6)
M (6)
A (7)
A (7)
■ No diabetes
17.
■ Intermediate- or high-risk findings on
M (6)
A (7)
A (7)
A (7)
A (7)
A (8)
A (8)
A (8)
noninvasive testing
■ No diabetes
18.
■ Low-risk findings on noninvasive testing
M (4)
M (6)
M (5)
M (6)
M (6)
A (7)
A (7)
A (8)
■ Diabetes present
19.
■ Intermediate- or high-risk findings on
M (6)
A (7)
M (6)
A (8)
A (7)
A (8)
A (7)
A (9)
noninvasive testing
■ Diabetes present
Intermediate or High Disease Complexity (e.g. Multiple Features of Complexity as Noted Previously, SYNTAX >22)
20.
■ Low-risk findings on noninvasive testing
M (4)
M (6)
M (4)
A (7)
M (5)
A (7)
M (6)
A (8)
■ No diabetes
21.
■ Intermediate- or high-risk findings on
M (5)
A (7)
M (6)
A (7)
M (6)
A (8)
M (6)
A (9)
noninvasive testing
■ No diabetes
22.
■ Low-risk findings on noninvasive testing
M (4)
A (7)
M (4)
A (7)
M (5)
A (8)
M (6)
A (9)
■ Diabetes present
23.
■ Intermediate- or high-risk findings on
M (4)
A (8)
M (5)
A (8)
M (5)
A (8)
M (6)
A (9)
noninvasive testing
■ Diabetes present
The number in parentheses next to the rating reflects the median score for that indication.
A indicates appropriate; AA, antianginal; BB, beta blockers; CABG, coronary artery bypass graft; M, may be appropriate; PCI, percutaneous coronary intervention; and SYNTAX, Synergy between
PCI with Taxus and Cardiac Surgery trial.
first modality to assess ambiguous left main severity, and
be particularly challenging because of the usual marked
the criteria for a significant stenosis are the same as for
size difference between the SVG and native artery.
non-left main stenosis (21,36,37).
Although FFR measurements are well-validated in
native vessels, data on the use of FFR in vein grafts are
limited
(38). After CABG surgery, the bypass conduit
Patients with prior CABG surgery can present with a wide
should act in a similar fashion to the native, low-
spectrum of disease progression. This includes the
resistance epicardial vessel. However, the assessment
development of new obstructive disease in coronary ar-
of ischemia due to a stenosis in a vein graft is compli-
teries not bypassed in the first operation, new stenoses in
cated by several features, which include: 1) the poten-
existing bypass grafts, and territory previously bypassed
tial for competing flow
(and pressure) from both the
but jeopardized again because of graft occlusion. Devel-
native and conduit vessels; 2) the presence of collaterals
oping indications inclusive of all of these anatomic pos-
from longstanding native coronary occlusion; and 3) the
sibilities would be impractical. Accordingly, the writing
potential for microvascular abnormalities due to
committee adopted a more compact construct based on
ischemic fibrosis and scarring, pre-existing or bypass
the presence of a significant stenosis in a bypass graft or
surgery-related myocardial infarction, or chronic low-
native coronary artery supplying
1,
2, or
3
distinct
flow ischemia. Despite these complicating features, the
vascular territories roughly corresponding to the terri-
theory of FFR should apply equally to both a lesion in
tories of the
3 main coronary arteries. As in patients
an SVG to the right coronary artery feeding a normal
without prior CABG, the indications included an assess-
myocardial bed and a lesion in the native right coro-
ment of risk based on noninvasive testing (low versus
nary. However, if the native and collateral supply
intermediate or high risk).
are sufficiently large, the FFR across an SVG stenosis
Evaluation of the severity and physiological signifi-
could be normal. FFR measurements may be most
cance of a stenosis in saphenous vein grafts (SVG) can
useful in the setting of an occluded bypass graft to a
16
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
TABLE 1.4
Left Main Coronary Artery Stenosis
Appropriate Use Score (1-9)
Left Main Disease
Asymptomatic
Ischemic Symptoms
Not on AA
Therapy or With
Not on AA
On 1 AA Drug
AA Therapy
Therapy
(BB Preferred)
On ≥2 AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
24.
■ Isolated LMCA disease
M (6)
A (8)
A (7)
A (8)
A (7)
A (9)
A (7)
A (9)
■ Ostial or midshaft stenosis
25.
■ Isolated LMCA disease
M (5)
A (8)
M (5)
A (8)
M (5)
A (9)
M (6)
A (9)
■ Bifurcation involvement
26.
■ LMCA disease
M (6)
A (8)
M (6)
A (9)
A (7)
A (9)
A (7)
A (9)
■ Ostial or midshaft stenosis
■ Concurrent multivessel disease
■ Low disease burden (e.g., 1-2 additional focal
stenoses, SYNTAX score #22)
27.
■ Ostial or midshaft stenosis
M (4)
A (9)
M (4)
A (9)
M (4)
A (9)
M (4)
A (9)
■ Concurrent multivessel disease
■ Intermediate or high disease burden (e.g., 1-2
additional bifurcation stenosis, long stenoses,
SYNTAX score >22)
28.
■ LMCA disease
M (4)
A (8)
M (5)
A (8)
M (5)
A (9)
M (6)
A (9)
■ Bifurcation involvement
■ Low disease burden in other vessels (e.g., 1-2
additional focal stenosis, SYNTAX score #22)
29.
■ LMCA disease
R (3)
A (8)
R (3)
A (9)
R (3)
A (9)
R (3)
A (9)
■ Bifurcation involvement
■ Intermediate or high disease burden in other
vessels (e.g., 1-2 additional bifurcation ste-
nosis, long stenoses, SYNTAX score >22)
The number in parentheses next to the rating reflects the median score for that indication.
A indicates appropriate; AA, antianginal; BB, beta blockers; CABG, coronary artery bypass graft; LMCA, left main coronary artery; M, may be appropriate; PCI, percutaneous coronary
intervention; R, rarely appropriate; and SYNTAX, Synergy between PCI with Taxus and Cardiac Surgery trial.
native artery with an intermediate-severity stenosis.
in the presence of a patent and fully functional IMA graft,
FFR measurements in bypass grafts are less well-
especially to the LAD. The path of the IMA, particularly if
validated and should thus be interpreted with caution.
it courses medially or is adherent to the back of the ster-
Two tables are presented for the rating of patients with
num, may be at greater risk during sternal re-entry, with
prior CABG depending on the patency of an existing in-
adverse consequences even if the IMA-grafted vessel is
ternal mammary artery (IMA) graft. IMAs have a greater
long-term patency rate than SVGs—typically >90% after
significantly diseased at the time of the original opera-
10 years (39,40). Accordingly, use of the IMA as a conduit
tion. Therefore, if the IMA to the LAD is no longer patent
in CABG surgery has steadily increased. Current use is
or is severely diseased, it is assumed that the native LAD
98%, as reported in the Society of Thoracic Surgeons na-
is also severely diseased or occluded.
tional database, and use of the IMA as a conduit is 1 of the
quality metrics in their composite score. Because of the
current high use of the IMA, the writing committee felt
Coronary Revascularization May Be Considered
there were too few patients to consider a separate cate-
In an effort to capture common clinical scenarios that are
gory consisting of patients who only had SVGs used in
not well-represented in guidelines, the writing group
their first operation, although a few such patients may
developed indications for preoperative revascularization
exist. Moreover, the writing committee did not develop
in patients being evaluated for renal transplantation or
any scenarios where the initial operation consisted of
structural heart procedures. The writing committee
only bypass grafts to the circumflex and right coronary
recognized that pre-operative revascularization is some-
artery in the absence of LAD disease. The patency and
times requested before transplantation of other organs,
longevity of the IMA as a bypass graft was felt by the
but there is insufficient experience or data from
writing committee to be an important decision point in
controlled studies upon which to develop meaningful
the indication development, as many cardiovascular sur-
scenarios. These scenarios do not capture all possible
geons are hesitant to perform a second bypass operation
clinical situations, but were felt to capture the majority of
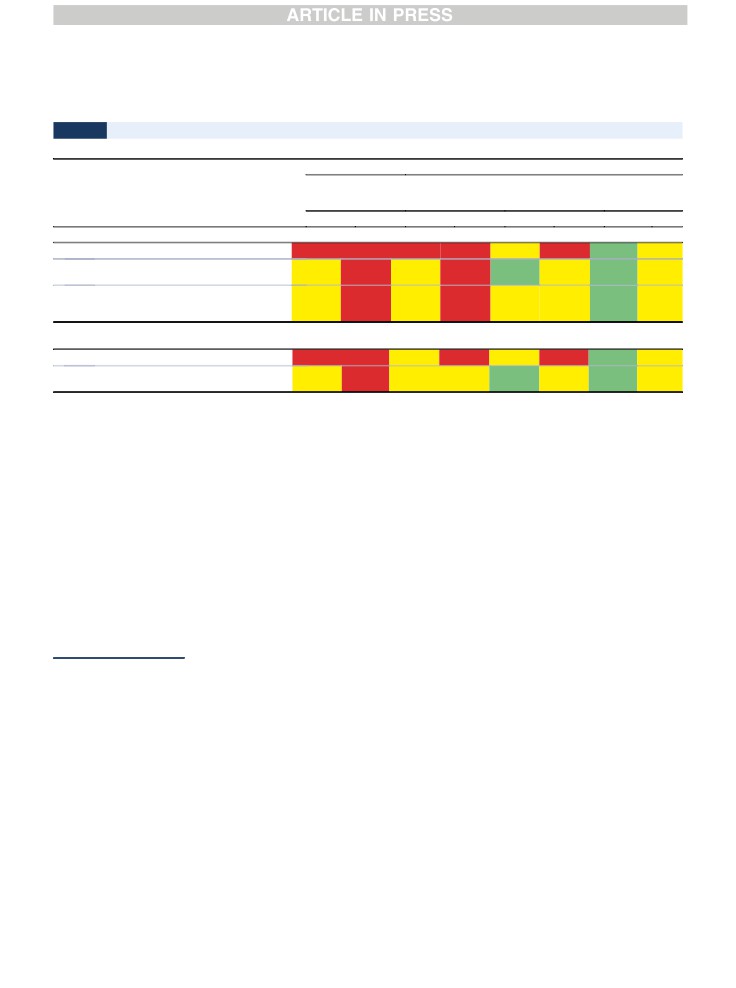
JACC VOL.
■, NO. ■, 2017
Patel et al.
17
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
TABLE 2.1
IMA to LAD Patent and Without Significant Stenoses
Appropriate Use Score (1-9)
Asymptomatic
Ischemic Symptoms
Not on AA
Therapy or With
Not on AA
On 1 AA Drug
AA Therapy
Therapy
(BB Preferred)
On ≥2 AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
Stenosis Supplying 1 Territory Disease (Bypass Graft or Native Artery) to Territory Other Than Anterior
30.
■ Low-risk findings on noninvasive testing
R (3)
R (1)
R (3)
R (2)
M (6)
R (3)
A (7)
M (4)
31.
■ Intermediate- or high-risk findings on
M (5)
R (3)
M (5)
R (3)
A (7)
M (4)
A (8)
M (5)
noninvasive testing
32.
■ No stress test performed or, if performed, the
M (4)
R (3)
M (4)
R (3)
M (6)
M (4)
A (8)
M (5)
results are indeterminate
■ FFR of stenosis #0.80*
Stenoses Supplying 2 Territories (Bypass Graft or Native Artery, Either 2 Separate Vessels or Sequential Graft Supplying 2 Territories) Not Including Anterior
Territory
33.
■ Low-risk findings on noninvasive testing
R (3)
R (2)
M (4)
R (3)
M (6)
R (3)
A (7)
M (5)
34.
■ Intermediate- or high-risk findings on
M (5)
R (3)
M (5)
M (4)
A (7)
M (5)
A (8)
M (6)
noninvasive testing
The number in parentheses next to the rating reflects the median score for that indication. *iFR measurements with appropriate normal ranges may be substituted for FFR.
A indicates appropriate; AA, Antianginal; BB, beta blockers; CABG, coronary artery bypass graft; FFR, fractional flow reserve; iFR, instant wave-free ratio; IMA, internal mammary artery; LAD, left
anterior descending coronary artery; M, may be appropriate; PCI, percutaneous coronary intervention; and R, rarely appropriate.
common clinical situations. If patients have an acute
5 cardiac surgeons, 5 interventional cardiologists, 6 cardi-
coronary syndrome, the writing group felt they should
ologists not directly involved with performing revascu-
be rated according to the AUC for acute coronary syn-
larization, and
1
outcomes researcher. Third, the new
drome. For many of these patients, symptoms may be
criteria stratify symptoms into
2
general group-
difficult to attribute to myocardial ischemia; thus, the
s—asymptomatic and ischemic symptoms—to be inclusive
indications used in this table provide only anatomic and
of the spectrum of complaints that may occur from
noninvasive test findings for review. Note that for pa-
myocardial ischemia. Furthermore, because of the variety
tients being evaluated before a percutaneous valve pro-
of symptoms that may indicate myocardial ischemia, in-
cedure, the option for CABG surgery is blocked out, as it is
dividual patient variation in how they are described, and
assumed such patients have clinical factors making their
observer variability in the assessment of symptom
risk of surgery prohibitively high.
severity, the writing group chose to abandon the Canadian
Cardiac Society classification. However, the current
7. DISCUSSION
criteria continue to emphasize the use of more objective
measures of ischemia within indications to stratify pa-
The AUC are intended to inform clinicians, patients, and
tients into low-risk or intermediate-/high-risk findings, as
health policy makers about the reasonable use of tech-
described in the SIHD guideline. Fourth, the scenarios
nologies to help improve patient symptoms and health
expand the use of intracoronary physiological testing,
outcomes. Since 2005, the American College of Cardiol-
mainly with FFR. Fifth, the structure of the AUC tables
ogy, along with its professional partners, has worked to
concerning the use of antianginal therapy has changed to
provide criteria for both invasive and noninvasive testing
reflect typical practice patterns rating patients on the basis
and selected treatments, with the intention of further
of no antianginal therapy, use of 1 antianginal drug, or use
expanding the AUC portfolio.
of 2 or more antianginal drugs. As in earlier documents, it is
The 2017 Appropriate Use Criteria for Revascularization
assumed that all patients are being treated with guideline-
in Patients With Stable Ischemic Heart Disease is the
directed medical therapies to reduce risk. Finally, in an
culmination of approximately 2 years of review and revi-
effort to capture patients who have not previously been
sion to the existing AUC. In response to comments from
categorized, the current AUC also rate coronary revascu-
multiple stakeholders, the current AUC has several
larization in patients being considered for renal trans-
important changes (41). First, this document will use the
plantation and percutaneous valve procedures.
new terms “appropriate care,” “may be appropriate care,”
Review of the ratings demonstrate some themes
and “rarely appropriate care,” which were described in the
around revascularization of patients with SIHD that are
updated AUC methodology paper (2). Second, the compo-
consistent with existing clinical practice guidelines. In
sition of the rating panel was changed slightly to include
general, in patients with a low burden of coronary disease

18
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
TABLE 2.2
IMA to LAD Not Patent
Appropriate Use Score (1-9)
Asymptomatic
Ischemic Symptoms
Not on AA
Therapy or With
Not on AA
On 1 AA Drug
AA Therapy
Therapy
(BB Preferred)
On ≥2 AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
Stenosis Supplying 1-Territory Disease (Bypass Graft or Native Artery)-Anterior (LAD) Territory
35.
■ Low-risk findings on noninvasive testing
M (4)
R (3)
M (5)
R (3)
M (6)
M (4)
A (7)
M (5)
36.
■ Intermediate- or high-risk findings on
M (6)
M (4)
M (6)
M (4)
A (7)
M (5)
A (8)
M (6)
noninvasive testing
37.
■ No stress test performed or, if performed, the
M (5)
M (4)
M (6)
M (4)
A (7)
M (5)
A (8)
M (6)
results are indeterminate
■ FFR of stenosis #0.80*
Stenoses Supplying 2 Territories (Bypass Graft or Native Artery, Either 2 Separate Vessels or Sequential Graft Supplying 2 Territories) LAD Plus Other Territory
38.
■ Low-risk findings on noninvasive testing
M (5)
M (4)
M (6)
M (4)
A (7)
M (5)
A (7)
M (6)
39.
■ Intermediate- or high-risk findings on
M (6)
M (5)
A (7)
M (6)
A (7)
A (7)
A (8)
A (8)
noninvasive testing
Stenoses Supplying 3 Territories (Bypass Graft or Native Arteries, Separate Vessels, Sequential Grafts, or Combination Thereof) LAD Plus 2 Other Territories
40.
■ Low-risk findings on noninvasive testing
M (5)
M (5)
M (6)
M (5)
M (6)
M (6)
A (7)
A (7)
41.
■ Intermediate- or high-risk findings on
A (7)
A (7)
A (7)
A (7)
A (7)
A (7)
A (8)
A (8)
noninvasive testing
The number in parentheses next to the rating reflects the median score for that indication. *iFR measurements with appropriate normal ranges may be substituted for FFR.
A indicates appropriate; AA, Antianginal; BB, beta blockers; CABG, coronary artery bypass graft; FFR, fractional flow reserve; iFR, instant wave-free ratio; IMA, internal mammary artery; LAD, left
anterior descending coronary artery; M, may be appropriate; PCI, percutaneous coronary intervention; and R, rarely appropriate.
(e.g., single-vessel disease), low-risk findings on nonin-
the majority of patients being evaluated before a percu-
vasive testing, and/or no antianginal therapy, revascu-
taneous valve procedure.
larization by PCI or CABG surgery for care is felt to be
rarely appropriate as the initial step. As disease burden
Application of Criteria
progresses through
2-vessel to
3-vessel and left main
There are many potential applications for AUC, including
disease, revascularization by PCI or CABG frequently be-
their adoption by Centers for Medicare & Medicaid Ser-
comes rated as “may be appropriate care” or “appropriate
vices regulators as a means of evaluating care. Clinicians
care,” with CABG surgery consistently rated as “appro-
can use the ratings for decision support or as an educa-
priate care” for intermediate or high disease complexity
tional tool when considering the need for revasculariza-
(SYNTAX ≥22) even in patients with ischemic symptoms
tion. Moreover, these criteria can be used to facilitate
who are not on antianginal therapy. Of note, CABG sur-
discussions with patients and/or referring physicians
gery was consistently rated as “appropriate care” and PCI
about the need for revascularization. The original intent
as “rarely appropriate care” for left main bifurcation dis-
of the AUC was to provide a tool to identify patterns of
ease with intermediate or high disease burden in other
care, including both the overuse and underuse of various
vessels.
services. In fact, some of the initial publications related to
Repeat CABG surgery was felt to be rarely appropriate
AUC identified underuse and the consequences of
in patients with a functional patent IMA to the LAD in all
underuse rather than overuse of services (42,43). Facil-
but 1 indication, with both PCI and CABG being rated as
ities have used these criteria to design protocols to facil-
either “may be appropriate care” or “appropriate care” in
itate the appropriate care of patients. Some payers have
the other indications, reflecting the complex and indi-
adopted the AUC for use in the preauthorization of pro-
vidualized decision making required in these patients.
cedures or retrospectively for quality reports. Although
With the exception of a few specific scenarios in asymp-
the AUC were never intended to determine payment in
tomatic patients with a low disease burden, revasculari-
individual patients, some payers have adopted the AUC
zation options were considered as “may be appropriate
for this purpose. The desire of payers to control costs is
care” or “appropriate care” options. Although not directly
understood, but it should be in the context of developing
rated, the use of fractional flow reserve for evaluation of
rational payment management strategies to ensure their
renal transplant patients may be considered and will be
members receive necessary, beneficial, and cost-effective
addressed in future revascularization documents. Revas-
cardiovascular care, rather than for other purposes. It is
cularization by PCI was considered appropriate care for
expected that services performed for “appropriate” or
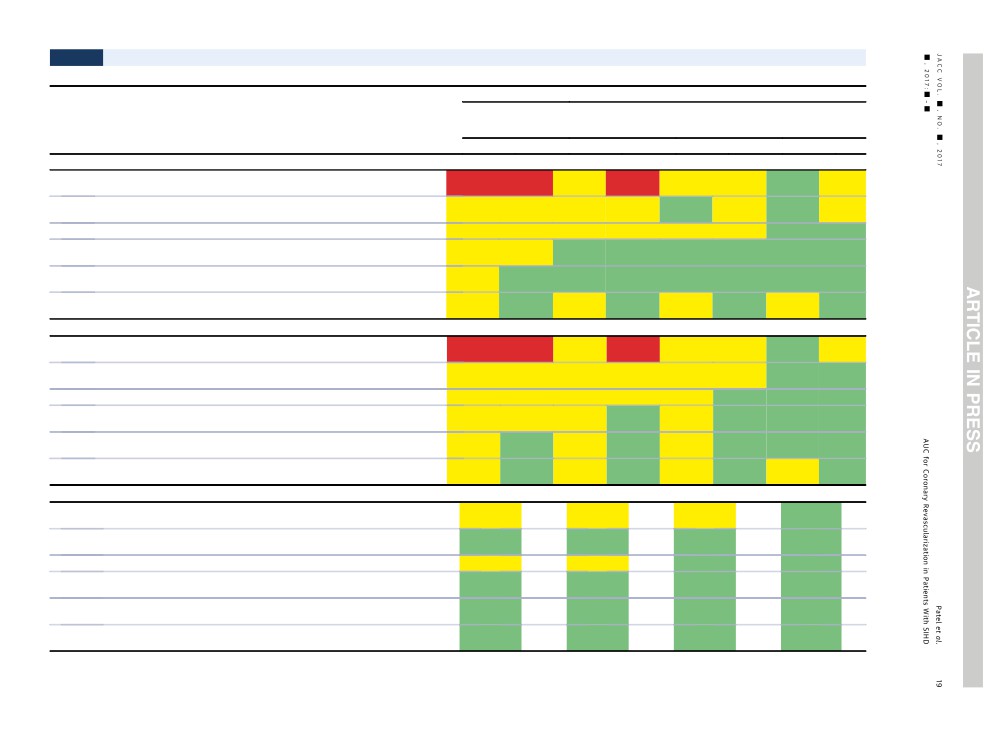
TABLE 3.1
Stable Ischemic Heart Disease Undergoing Procedures for Which Coronary Revascularization May Be Considered
Appropriate Use Score (1-9)
Asymptomatic
Ischemic Symptoms
Not on AA Therapy
or With AA
On 1 AA Drug
Therapy
Not on AA Therapy
(BB Preferred)
On ≥2 AA Drugs
Indication
PCI
CABG
PCI
CABG
PCI
CABG
PCI
CABG
Patients Undergoing Renal Transplantation, No Diabetes
42.
■ One- or two-vessel CAD, no proximal LAD involvement, with low-risk noninvasive
R (3)
R (2)
M (4)
R (3)
M (6)
M (4)
A (7)
M (5)
findings
43.
■ One- or two-vessel CAD, no proximal LAD involvement, with intermediate- or high-risk
M (5)
M (4)
M (6)
M (4)
A (7)
M (5)
A (8)
M (6)
noninvasive findings
44.
■ One- or two-vessel CAD, including proximal LAD, with low-risk noninvasive findings
M (5)
M (4)
M (6)
M (5)
M (6)
M (6)
A (8)
A (7)
45.
■ One- or two-vessel CAD, including proximal LAD, with intermediate- or high-risk
M (6)
M (6)
A (7)
A (7)
A (7)
A (7)
A (8)
A (8)
noninvasive findings
46.
■ Left main and/or three-vessel disease, with intermediate- or high-risk noninvasive
M (6)
A (7)
A (7)
A (7)
A (7)
A (7)
A (8)
A (8)
findings (e.g., SYNTAX #22)
47.
■ Left main and/or three-vessel disease, with intermediate- or high-risk noninvasive
M (5)
A (7)
M (6)
A (8)
M (6)
A (8)
M (6)
A (9)
findings (e.g., SYNTAX >22)
Patients Undergoing Renal Transplantation, Diabetes Present
48.
■ One- or two-vessel CAD, no proximal LAD involvement, with low-risk noninvasive
R (3)
R (3)
M (4)
R (3)
M (5)
M (4)
A (7)
M (6)
findings
49.
■ One- or two-vessel CAD, no proximal LAD involvement, with intermediate- or high-risk
M (5)
M (4)
M (5)
M (4)
M (6)
M (5)
A (7)
A (7)
noninvasive findings
50.
■ One- or two-vessel CAD, including proximal LAD, with low-risk noninvasive findings
M (5)
M (5)
M (5)
M (6)
M (5)
A (7)
A (7)
A (7)
51.
■ One- or two-vessel CAD, including proximal LAD, with intermediate- or high-risk
M (6)
M (6)
M (6)
A (7)
M (6)
A (7)
A (7)
A (8)
noninvasive findings
52.
■ Left main and/or three-vessel disease, with intermediate- or high-risk noninvasive
M (6)
A (8)
M (6)
A (8)
M (6)
A (8)
A (7)
A (9)
findings (e.g., SYNTAX #22)
53.
■ Left main and/or three-vessel disease, with intermediate- or high-risk noninvasive
M (5)
A (8)
M (5)
A (8)
M (5)
A (9)
M (5)
A (9)
findings (e.g., SYNTAX >22)
Patient Who Will Undergo a Percutaneous Valve Procedure (TAVR, MitraClip, Others)
54.
■ One- or two-vessel CAD, no proximal LAD involvement, with low-risk noninvasive
M (4)
M (4)
M (6)
A (8)
findings
55.
■ One- or two-vessel CAD, no proximal LAD involvement, with intermediate- or high-risk
A (7)
A (7)
A (7)
A (8)
noninvasive findings
56.
■ One- or two-vessel CAD, including proximal LAD, with low-risk noninvasive findings
M (6)
M (6)
A (7)
A (8)
57.
■ One- or two-vessel CAD, including proximal LAD, with intermediate- or high-risk
A (7)
A (7)
A (8)
A (9)
noninvasive findings
58.
■ Left main and/or three-vessel disease, with intermediate- or high-risk noninvasive
A (8)
A (8)
A (8)
A (9)
findings (e.g., SYNTAX #22)
59.
■ Left main and/or three-vessel disease, with intermediate- or high-risk noninvasive
A (7)
A (7)
A (8)
A (8)
findings (e.g., SYNTAX >22)
The number in parentheses next to the rating reflects the median score for that indication.
A indicates appropriate; AA, Antianginal; BB, beta blockers; CABG, coronary artery bypass graft; CAD, coronary artery disease; LAD, left anterior descending coronary artery; M, may be appropriate; PCI, percutaneous coronary intervention;
R, rarely appropriate; SYNTAX, Synergy between PCI with Taxus and Cardiac Surgery trial; and TAVR, transcatheter aortic valve replacement.
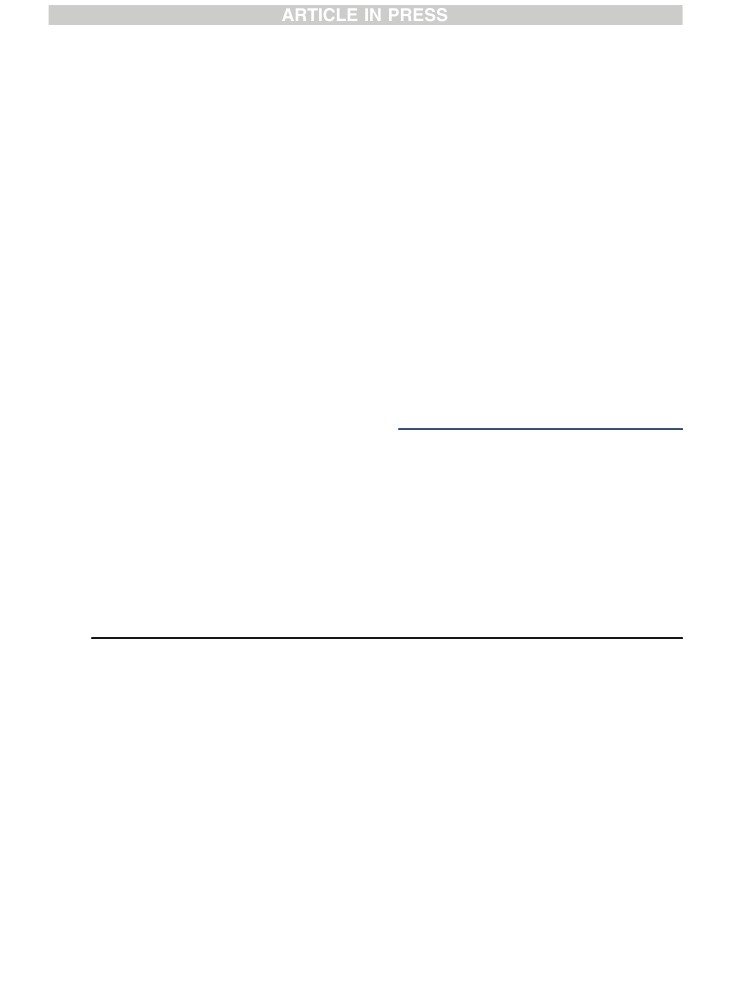
20
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
“may be appropriate” indications will receive reim-
transparent for all providers to review and implement
bursement. In contrast, services performed for “rarely
local systems of care.
appropriate” indications should be justified by additional
In conclusion, this document represents the current
documentation to justify payment because of the unique
understanding of the clinical benefit of coronary revascu-
circumstances or the clinical profile that must exist in
larization with respect to health outcomes and survival.
such a patient. It is critical to emphasize that the writing
These criteria have been developed through the AUC pro-
group, technical panel, Appropriate Use Criteria Task
cess and alignment with the evidence and recommenda-
Force, and clinical community do not believe a rating of
tions from clinical practice guidelines. This is intended to
“may be appropriate” is justification to deny reimburse-
provide a practical guide to clinicians and patients when
ment for revascularization. Rather, “may be appropriate”
considering revascularization. As with all AUC, some of
ratings are those in which the available data vary and
these ratings will require research and further evaluation
many other factors exist that may affect the decision to
to provide the greatest information and benefit to clinical
perform or not perform revascularization. The opinions of
decision making. We anticipate that the utility and ability
the technical panel often varied for these indications,
of these criteria to improve the quality of care will be
reflecting that additional research is needed.
measured by the overall use and adoption of the criteria.
The writing group recognizes the need to align the
With each update, the AUC for coronary revascularization
collection of clinical data required for the determination
in SIHD have become more refined and specific, while areas
of appropriate use with appropriate methods to reduce
for continued focus and research have been identified.
the burden of data collection. To this end, the NCDR
CathPCI Registry group has been engaged in a parallel
ACC PRESIDENT AND STAFF
process to ensure that needed data elements are incor-
porated into the Registry. The criteria will also be eval-
Richard A. Chazal, MD, FACC, President
uated for collection by the Society for Thoracic Surgeons
Shalom Jacobovitz, Chief Executive Officer
registry. Incorporating fields to identify patients who are
William J. Oetgen, MD, FACC, Executive Vice President,
not felt to be candidates for PCI or CABG surgery has
Science, Education and Quality
been suggested to ensure proper mapping of the AUC in
Joseph M. Allen, MA, Director, Team Leader, Clinical
the course of medical decision making. The writing
Policy and Pathways
committee believes the key step to ensuring that the
Leah White, MPH, CCRP, Team Leader, Appropriate Use
AUC are iterated and continually improved is the use of
Criteria
a feedback cycle of data between current clinical practice
Marίa Velásquez, Senior Research Specialist, Appropriate
and the Registry. The writing group also believes that
Use Criteria
the mapping of the data elements on the NCDR CathPCI
Amelia Scholtz, PhD, Publications Manager, Clinical Pol-
Registry data collection from the AUC should be
icy and Pathways
REFERENCES
JACC VOL.
■, NO. ■, 2017
Patel et al.
21
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
KEY WORDS ACC Appropriate Use Criteria,
coronary artery bypass graft, coronary
revascularization, percutaneous coronary
intervention, stable ischemic heart disease
22
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
APPENDIX A. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 APPROPRIATE USE CRITERIA FOR
CORONARY REVASCULARIZATION IN PATIENTS WITH STABLE ISCHEMIC HEART DISEASE:
PARTICIPANTS
Writing Group
A&M Health Science Center College of Medicine; Vice-
President and Medical Director, Cardiovascular Services,
Manesh R. Patel, MD, FACC, FAHA, FSCAI—Associate
Central Texas Division, Baylor Scott & White-Temple
Professor of Medicine Director of Interventional Cardi-
Memorial, Temple, TX
ology and Catheterization Labs, Duke University
Peter K. Smith, MD, FACC, Writing Committee Liaison—
Health System, Duke Clinical Research Institute,
Professor of Surgery, Division Chief, Cardiovascular and
Durham, NC
Thoracic Surgery, Duke University, Durham, NC
John H. Calhoon, MD—Professor and Chair, President’s
James C. Blankenship, MD, MACC, FSCAI—Staff Physi-
Council Chair for Excellence in Surgery, Department of
cian, Director, Cardiac Catheterization Laboratory, Divi-
Cardiothoracic Surgery; Director, University of Texas
sion of Cardiology, Geisinger Medical Center, Danville, PA
Health Science Center at San Antonio, Heart and Vascular
Alfred A. Bove, MD, PhD, MACC— Past President,
Institute, San Antonio, TX
American College of Cardiology; Professor Emeritus,
Gregory J. Dehmer, MD, MACC, MSCAI, FAHA—Clinical
Lewis Katz School of Medicine, Heart and Vascular,
Professor of Medicine, Texas A&M Health Science Center
Temple University, Philadelphia, PA
College of Medicine; Vice-President and Medical Director,
Steven M. Bradley, MD—Staff Cardiologist, VA Eastern
Cardiovascular Services, Central Texas Division, Baylor
Scott & White-Temple Memorial, Temple, TX
Colorado Health Care System; Assistant Professor of
James Aaron Grantham, MD, FACC—Associate Clinical
Medicine, Division of Cardiology at the University of
Professor, University of Missouri-Kansas City School of
Colorado, Denver, CO
Medicine; Director, Cardiovascular Disease Fellowship
Larry S. Dean, MD, FACC, FSCAI—Professor of Medicine
Program, University of Missouri-Kansas City School of
and Surgery, University of Washington School of Medi-
Medicine; Director, Cardiovascular Medical Education,
cine; Director, University of Washington, Medicine
Saint Luke’s Hospital, Kansas City, MO
Regional Heart Center, Seattle, WA
Thomas M. Maddox, MD, MSc, FACC, FAHA—National
Peter L. Duffy, MD, FACC, FSCAI—Director of Quality
for the Cardiovascular Service Line, First Health of the
Director, VA CART Program Cardiology, VA Eastern Col-
Carolinas, Reid Heart Institute/Moore Regional Hospital,
orado Health Care System; Associate Professor, Depart-
Pinehurst North Carolina
ment of Medicine, Cardiology, University of Colorado,
T. Bruce Ferguson, Jr., MD, FACC—Professor of
Colorado Cardiovascular Outcomes Research Consortium,
Thoracic Surgery, Department of Cardiovascular Sciences,
Denver, CO
Cardiothoracic Surgery, East Carolina Heart Institute, East
David J. Maron, MD, FACC, FAHA—Clinical Professor of
Carolina University, Greenville, NC
Medicine, Cardiovascular; Director, Preventive Cardiol-
Frederick L. Grover, MD, FACC—Professor of Cardio-
ogy, Stanford University School of Medicine, Stanford, CA
thoracic Surgery, Department of Cardiothoracic Surgery,
Peter K. Smith, MD, FACC— Professor of Surgery, Divi-
University of Colorado, Denver, CO
sion Chief, Cardiovascular and Thoracic Surgery, Duke
Robert A. Guyton, MD, FACC—Chief of Cardiothoracic
University, Durham, NC
Surgery, Professor of Surgery, Division of Cardiothoracic
Surgery, Department of Surgery; Director, Thoracic Sur-
Rating Panel
gery Residency Program, Emory University School of
Manesh R. Patel, MD, FACC, FAHA, FSCAI, Writing Com-
Medicine, Atlanta, GA
mittee Liaison—Associate Professor of Medicine, Director
Mark A. Hlatky, MD, FACC—Professor of Heath
Interventional Cardiology and Catheterization Labs, Duke
Research and Policy, Health Services Research; Professor
University Health System, Duke Clinical Research Insti-
of Medicine, Cardiovascular Medicine, Stanford Univer-
tute, Durham, NC
sity School of Medicine, Stanford, CA
Michael J. Wolk, MD, MACC, Moderator—Past Presi-
Harold L. Lazar, MD, FACC—Director, Cardiothoracic
dent, American College of Cardiology; Clinical Professor
Research Program; Professor of Cardiothoracic Surgery,
of Medicine, Weill Medical College of Cornell University,
Boston University School of Medicine, Boston, MA
New York Cardiology Associates, New York, NY
Vera H. Rigolin, MD, FACC—Professor, Cardiology,
Gregory J. Dehmer, MD, MACC, MSCAI, FAHA, Writing
Northwestern University Feinberg School of Medicine,
Committee Liaison—Clinical Professor of Medicine, Texas
Chicago, IL

JACC VOL.
■, NO. ■, 2017
Patel et al.
23
■, 2017:■-■
AUC for Coronary Revascularization in Patients With SIHD
Geoffrey A. Rose, MD, FACC, FASE—Chief, Division of
Robert N. Piana, MD, FACC—Professor of Medicine, Car-
Cardiology, Sanger Heart and Vascular Institute, Char-
diology,VanderbiltUniversityMedicalCenter,Nashville,TN
lotte, NC
John A. Spertus, M.D, MPH, FACC—Adjunct Professor of
Richard J. Shemin, MD, FACC—Robert and Kelly Day
Medicine, Washington University School of Medicine,
Professor, Chief of Cardiothoracic Surgery, Executive Vice
Saint Louis, MO
Chair of Surgery, Co-Director of the Cardiovascular Cen-
Raymond F. Stainback, MD, FACC— Medical Director,
ter, Director of Cardiac Quality at the Ronald Reagan
Non-Invasive Cardiology Texas Heart Institute at Baylor
UCLA Medical Center, Los Angeles, CA
St. Luke’s Medical Center, Houston, TX
Jacqueline E. Tamis-Holland, MD, FACC—Director,
Robert C. Stoler, MD, FACC—Director of Cardiac Cath-
Interventional Cardiology Fellowship, Mount Sinai; Saint
eterization Laboratory, Cardiology Consultants of Texas,
Luke’s Hospital Director, Women’s Heart NY Assistant
Dallas, TX
Professor of Medicine, Icahn School of Medicine at Mount
Todd C. Villines, MD, FACC—Co-Director of Cardiovas-
Sinai Hospital, New York, NY
cular Computed Tomography and Assistant Chief, Cardi-
Carl L. Tommaso, MD, FACC, FSCAI—Director, Cardiac
ology Service at Walter Reed Army Medical Center,
Catheterization Laboratory, Skokie Illinois Hospital, part
Rockville, MD
of the Northshore University Health System; Associate
David H. Wiener, MD, FACC—Professor of Medicine,
Professor of Medicine, Rush Medical College, Chicago, IL
Jefferson Medical College, Jefferson Heart Institute,
L. Samuel Wann, MD, MACC—Past President, American
Philadelphia, PA
College of Cardiology; Clinical Cardiologist, Columbia St.
Mary’s Healthcare; Medical Director, Heart Failure Pro-
ACC Appropriate Use Criteria Task Force
gram, Milwaukee, WI
Steven R. Bailey, MD, FACC, FSCAI, FAHA—Chair, Divi-
John B. Wong, MD—Chief, Division of Clinical Decision
sion of Cardiology; Professor of Medicine and Radiology,
Making, Primary Care Physician, Principal Investigator,
Janey Briscoe Distinguished Chair, University of Texas
Institute for Clinical Research and Health Policy Studies;
Health Sciences Center, San Antonio, TX
Professor, Tufts University School of Medicine, Boston, MA
Nicole Bhave, MD, FACC—Clinical Assistant Professor,
Department of Internal Medicine, Division of Cardiovas-
Reviewers
cular Medicine, University of Michigan Cardiovascular
Jeffrey L. Anderson, MD, FACC—Associate Chief of
Center, Ann Arbor, MI
Cardiology, Intermountain Medical Center, Murray, UT
Alan S. Brown, MD, FACC—Medical Director, Midwest
James C. Blankenship, MD, MACC, MSCAI—Staff
Heart Disease Prevention Center, Advocate Lutheran
Physician, Director, Cardiac Catheterization Laboratory,
General Hospital; Director, Division of Cardiology, Park
Geisinger Medical Center, Division of Cardiology,
Ridge, IL
Danville, PA
Stacie L. Daugherty, MD, FACC—Associate Professor,
Jeffrey A. Brinker, MD, FACC—Professor of Medicine,
Division of Cardiology, Department of Medicine, Univer-
Johns Hopkins Hospital, Baltimore, MD
sity of Colorado School of Medicine, Denver, CO
Alexandru I. Costea, MD—Associate Professor, Univer-
Gregory J. Dehmer, MD, MACC, MSCAI, FAHA—
sity of Cincinnati Medical Center, Cincinnati, OH
Co-Chair, AUC Task Force, Clinical Professor of Medicine,
Ali E. Denktas, MD, FACC—Assistant Professor, Baylor
Texas A&M Health Science Center College of Medicine;
College of Medicine, Houston, TX
Vice President and Medical Director, Cardiovascular
Lloyd W. Klein, MD, FACC—Professor of Medicine,
Services, Central Texas Division, Baylor Scott and White-
Melrose Park, IL
Temple Memorial, Temple, TX
Frederick G. Kushner, MD, FACC—Clinical Professor,
Milind Y. Desai, MBBS, FACC—Associate Director,
Tulane University Medical Center; Medical Director, Heart
Clinical Investigations Heart and Vascular Institute,
Clinic of Louisiana, Marrero, LA
Cleveland Clinic, Cleveland, OH
Glenn N. Levine, MD, FACC—Professor, Baylor College
John U. Doherty, MD, FACC, FAHA—Co-Chair, AUC Task
of Medicine, Cardiology, Pearland, TX
Force, Professor of Medicine, Jefferson Medical College of
David Joel Maron, MD, FACC—Professor of Medicine
Thomas Jefferson University, Philadelphia, PA
and Emergency Medicine, Stanford University School of
Claire Duvernoy, MD, FACC—Cardiology Section Chief,
Medicine, Stanford, CA
Division of Cardiology, University of Michigan Health
James B. McClurken, MD, FACC—Director of
System, Ann Arbor, MI
Thoracic Surgery, Professor of Surgery Emeritus, Temple
Linda D. Gillam, MD, FACC—Chair, Department of Car-
University, School of Medicine, Richard A Reif Heart
diovascular Medicine, Morristown Medical Center, Mor-
Institute, Doylestown Hospital, Doylestown, PA
ristown, NJ
24
Patel et al.
JACC VOL.
■, NO. ■, 2017
AUC for Coronary Revascularization in Patients With SIHD
■, 2017:■-■
Robert C. Hendel, MD, FACC, FAHA, FASNC—Director
David E. Winchester, MD, FACC—Assistant Professor of
of Cardiac Imaging and Outpatient Services, Division
Medicine, University of Florida, Division of Cardiology,
of Cardiology, Miami University School of Medicine,
Gainesville, FL
Miami, FL
Joseph M. Allen, MA—Team Leader, Clinical Policy and
Christopher M. Kramer, MD, FACC, FAHA—Former Co-
Pathways, American College of Cardiology, Washington, DC
Chair, AUC Task Force, Ruth C. Heede Professor of Car-
diology & Radiology; Director, Cardiovascular Imaging
APPENDIX B. RELATIONSHIPS WITH INDUSTRY
Center, University of Virginia Health System, Charlottes-
AND OTHER ENTITIES
ville, VA
Bruce D. Lindsay, MD, FACC—Professor of Cardiology,
The College and its partnering organizations rigorously
Cleveland Clinic Foundation of Cardiovascular Medicine,
avoid any actual, perceived, or potential conflicts of in-
Cleveland, OH
terest that might arise as a result of an outside relationship
Warren J. Manning, MD, FACC—Professor of Medicine
or personal interest of a member of the rating panel. Spe-
and Radiology, Beth Israel Deaconess Medical Center,
cifically, all panelists are asked to provide disclosure
Division of Cardiology, Boston, MA
statements of all relationships that might be perceived as
Manesh R. Patel, MD, FACC— Former Chair, AUC Task
real or potential conflicts of interest. These statements
Force; Assistant Professor of Medicine, Division of Car-
were reviewed by the Appropriate Use Criteria Task Force,
diology, Duke University Medical Center, Durham, NC
discussed with all members of the rating panel at the face-
Ritu Sachdeva, MD, FACC—Associate Professor, Division
to-face meeting, and updated and reviewed as necessary.
of Pediatric Cardiology, Department of Pediatrics, Emory
The following is a table of relevant disclosures by the rating
University School of Medicine, Children’s Health Care of
panel and oversight working group members. In addition,
Atlanta, Sibley Heart Center Cardiology, Atlanta, GA
to ensure complete transparency, a full list of disclosure
L. Samuel Wann, MD, MACC—Staff Cardiologist,
information—including relationships not pertinent to this
Columbia St. Mary’s Healthcare, Milwaukee, WI
APPROPRIATE USE CRITERIA FOR CORONARY REVASCULARIZATION IN PATIENTS WITH STABLE ISCHEMIC HEART DISEASE:
MEMBERS OF THE WRITING GROUP, RATING PANEL, INDICATION REVIEWERS, AND AUC TASK FORCE—
RELATIONSHIPS WITH INDUSTRY AND OTHER ENTITIES (RELEVANT)
Institutional,
Ownership/
Organizational,
Speakers
Partnership/
or Other Financial
Expert
Participant
Employment
Consultant
Bureau
Principal
Personal Research
Benefit
Witness
Manesh R. Patel
Duke University Health System, Duke
None
None
None
None
None
None
(Chair)
Clinical Research Institute—Associate
Professor of Medicine, Director,
Interventional Cardiology and
Catheterization Labs
John H. Calhoon
University of Texas Health Science Center
None
None
None
None
None
None
at San Antonio, Department of
Cardiothoracic Surgery, Heart and Vascular
Institute—Director, Professor, and Chair,
Presidents Council Chair for Excellence in
Surgery
Gregory J. Dehmer
Baylor Scott & White-Temple Memorial,
None
None
None
None
None
None
Texas A&M Health Science Center College
of Medicine, Central Texas Division—Clinical
Professor of Medicine, Medical Director,
Cardiovascular Services, Director,
Cardiology Division
James Aaron
Saint Luke’s Hospital—Associate Clinical
■
Abbott Vascular*
None
None
■
Abbott Vascular*
None
None
Grantham
Professor, University of Missouri-Kansas
■
Asahi-Intecc*
■
Asahi-Intecc*
City School of Medicine—Director,
■
Boston Scientific*
■
Boston Scientific*
Cardiovascular Disease Fellowship
■
Bridgepoint Medical
■
Bridgepoint Medical
Program, Director, Cardiovascular Medical
Systems*
Systems*
Education
■
Medtronic*
■
Medtronic*
Thomas M. Maddox
VA Eastern Colorado Health Care System—
None
None
None
None
None
None
National Director, Associate Professor,
Department of Medicine, Cardiology,
University of Colorado, Colorado
Cardiovascular Outcomes Research
Consortium
David J. Maron
Stanford University School of Medicine—
None
None
None
None
None
None
Clinical Professor of Medicine,
Cardiovascular, Director, Preventive
Cardiology
Peter K. Smith
Cardiovascular and Thoracic Surgery, Duke
None
None
None
None
None
None
University—Professor of Surgery, Division
Chief
Continued on the next page
APPENDIX B. CONTINUED
Institutional,
Ownership/
Organizational,
Speakers
Partnership/
or Other Financial
Expert
Participant
Employment
Consultant
Bureau
Principal
Personal Research
Benefit
Witness
Rating Panel
James C. Blankenship
Geisinger Medical Center, Division of
None
None
None
■
Abbott Vascular†
None
None
Cardiology—Staff Physician, Director,
■
AstraZeneca†
Cardiac Catheterization Laboratory
■
Boston Scientific†
■
GlaxoSmithKline†
■
Hamilton Health
Services†
■
Medinal LTD*
■
Orexigen Therapeu-
tics/Takeda†
■
Stentys, Inc.†
■
Takeda
Pharmaceuticals
Alfred A. Bove
Temple University, Lewis Katz School of
None
None
None
■
Merck Schering-
None
None
Medicine, Heart and Vascular—Professor
Plough†
Emeritus
Steven M. Bradley
VA Eastern Colorado Health Care System,
None
None
None
None
None
None
Division of Cardiology at the University of
Colorado—Staff Cardiologist, Assistant
Professor of Medicine
Larry S. Dean
Medicine Regional Heart Center University
■
Philips Medical*
None
None
■
Edwards
None
None
of Washington School of Medicine—
Lifesciences*
Professor of Medicine and Surgery, Director
Peter L. Duffy
First Health of the Carolinas, Reid Heart
None
■
Volcano Corp*
None
None
None
None
Institute/Moore Regional Hospital—
Director of Quality for the Cardiovascular
Service Line
T. Bruce Ferguson, Jr.
East Carolina Heart Institute, East Carolina
None
None
■
RFPi†
■
Novadaq
None
None
University, Department of Cardiovascular
Technologies*
Sciences, Cardiothoracic Surgery—Professor
of Thoracic Surgery
Frederick L. Grover
University of Colorado, Department of
■
Somalution
None
None
None
None
None
Cardiothoracic Surgery—Professor of
Cardiothoracic Surgery
Robert A. Guyton
Emory University School of Medicine,
■
Medtronic*
None
None
None
None
None
Division of Cardiothoracic Surgery,
Department of Surgery, Thoracic Surgery
Residency Program—Chief of
Cardiothoracic Surgery, Professor of
Surgery Director
Mark A. Hlatky
Stanford University School of Medicine,
None
None
None
None
■
Sanofi-Aventis
None
Cardiovascular Medicine, Health Services
Research—Professor of Heath Research and
Policy, Professor of Medicine
Continued on the next page
APPENDIX B. CONTINUED
Institutional,
Ownership/
Organizational,
Speakers
Partnership/
or Other Financial
Expert
Participant
Employment
Consultant
Bureau
Principal
Personal Research
Benefit
Witness
Harold L. Lazar
Boston University School of Medicine,
None
None
None
None
None
None
Cardiothoracic Research Program—Director
Professor of Cardiothoracic Surgery
Vera H. Rigolin
Northwestern University Feinberg School
None
None
None
None
■
Pfizer*
None
of Medicine, Cardiology—Professor
Geoffrey A. Rose
Division of Cardiology, Sanger Heart and
None
None
None
None
■
Medtronic
None
Vascular Institute—Chief
Richard J. Shemin
Ronald Reagan UCLA Medical Center,
■
Edwards Lifesciences
None
None
None
None
None
Cardiovascular Center—Director of Cardiac
■
Sorin Group
Quality, Robert and Kelly Day Professor,
Chief of Cardiothoracic Surgery, Executive
Vice Chair of Surgery
Jacqueline E.
Saint Luke’s Hospital, Icahn School of
None
None
None
None
None
None
Tamis-Holland
Medicine at Mount Sinai Hospital Mount
Sinai—Director, Women’s Heart NY,
Assistant Professor of Medicine, Director,
Interventional Cardiology Fellowship
Carl L. Tommaso
Rush Medical College in Chicago, Skokie
None
None
None
None
None
None
Illinois Hospital, part of the Northshore
University Health System—Director of the
Cardiac Catheterization Laboratory,
Associate Professor of Medicine
L. Samuel Wann
Columbia St. Mary’s Healthcare—Clinical
■
United Healthcare
None
None
None
None
None
Cardiologist, Medical Director, Heart
Failure Program
John B. Wong
Tufts University School of Medicine—Chief,
None
None
None
None
None
None
Division of Clinical Decision Making,
Primary Care Physician, Principal
Investigator, Institute for Clinical Research
and Health Policy Studies, Professor
Reviewers
Jeffrey L. Anderson
Intermountain Medical Center—Associate
■
Medicines Company
None
None
None
None
None
Chief of Cardiology
■
Sanofi-Aventis
Jeffrey A. Brinker
Johns Hopkins Hospital—Professor of
None
None
None
None
None
None
Medicine
Alexandru I. Costea
University of Cincinnati Medical Center—
None
None
None
None
■
Boston
None
Associate Professor
Scientific†
Ali E. Denktas
Baylor College of Medicine—Assistant
None
None
None
■
AstraZeneca
None
None
Professor
■
Edwards Lifesciences
Continued on the next page
APPENDIX B. CONTINUED
Institutional,
Ownership/
Organizational,
Speakers
Partnership/
or Other Financial
Expert
Participant
Employment
Consultant
Bureau
Principal
Personal Research
Benefit
Witness
Lloyd W. Klein
Melrose Park—Professor of Medicine
None
None
None
None
None
None
Frederick G. Kushner
Tulane University Medical Center, Heart
None
None
None
None
None
None
Clinic of Louisiana—Clinical Professor,
Medical Director
Glenn N. Levine
Baylor College of Medicine, Cardiology—
None
None
None
None
None
None
Professor
David J. Maron
Stanford University School of Medicine—
None
None
None
None
None
None
Professor of Medicine and Emergency
Medicine
James B. McClurken
Temple University, School of Medicine,
None
None
None
None
None
None
Richard A Reif Heart Institute, Doylestown
Hospital—Director of Thoracic Surgery,
Professor of Surgery Emeritus
Robert N. Piana
Vanderbilt University Medical Center—
■
Axio Research
None
None
None
None
None
Professor of Medicine, Cardiology
■
Harvard Clinical
Research Institute
■
W.L. Gore & Associ-
ates, Inc.
John A. Spertus
Washington University School of
■
Amgen
None
■
Health Outcomes
None
None
None
Medicine—Adjunct Professor of Medicine
■
Bayer Healthcare
Sciences
Pharmaceuticals
■
Janssen
■
Novartis
■
Regeneron
Raymond F.
Texas Heart Institute at Baylor St. Luke’s
None
None
None
None
None
None
Stainback
Medical Center, Non-Invasive Cardiology—
Medical Director
Robert C. Stoler
Cardiology Consultants of Texas—Director
■
Boston Scientific
None
None
None
None
None
of Cardiac Catheterization Laboratory
■
Medtronic
Todd C. Villines
Cardiology Service at Walter Reed Army
■
Boehringer
None
None
None
None
None
Medical Center—Co-Director of
Ingelheim
Cardiovascular Computed Tomography and
Pharmaceutical*
Assistant Chief
David H. Wiener
Jefferson Medical College, Jefferson Heart
None
None
None
None
None
None
Institute—Professor of Medicine
Appropriate Use Criteria Task Force
Steven R. Bailey
University of Texas Health Sciences
None
None
None
None
None
None
Center—Chair, Division of Cardiology,
Professor of Medicine and Radiology, Janey
Briscoe Distinguished Chair
Continued on the next page
APPENDIX B. CONTINUED
Institutional,
Ownership/
Organizational,
Speakers
Partnership/
or Other Financial
Expert
Participant
Employment
Consultant
Bureau
Principal
Personal Research
Benefit
Witness
Nicole Bhave
University of Michigan Cardiovascular
None
None
None
None
None
None
Center, Department of Internal Medicine,
Division of Cardiovascular Medicine—
Clinical Assistant Professor
Alan S. Brown
Midwest Heart Disease Prevention Center,
None
None
None
None
None
None
Advocate Lutheran General Hospital—
Director, Division of Cardiology—Medical
Director
Stacie L. Daugherty
University of Colorado School of Medicine,
None
None
None
None
None
None
Division of Cardiology, Department of
Medicine—Associate Professor
Gregory J. Dehmer
Baylor Scott & White, Central Texas
None
None
None
None
None
None
Division, Cardiovascular Services Health—
Medical Director
Milind Y. Desai
Cleveland Clinic, Clinical Investigations,
None
None
None
None
None
None
Heart and Vascular Institute—Associate
Director
John U. Doherty
Thomas Jefferson University, Jefferson
None
None
None
None
None
None
Medical College—Professor of Medicine
Claire Duvernoy
University of Michigan Health System,
None
None
None
None
None
None
Division of Cardiology—Cardiology Section
Chief
Linda D. Gillam
Morristown Medical Center, Department of
■
Edwards
None
None
None
None
None
Cardiovascular Medicine—Chair
Lifesciences*
■
Medtronic†
Robert C. Hendel
Miami University School of Medicine,
None
None
None
None
None
None
Division of Cardiology—Director of Cardiac
Imaging and Outpatient Services
Christopher M.
University of Virginia Health System—Ruth
None
None
None
None
None
None
Kramer
C. Heede Professor of Cardiology &
Radiology, Director, Cardiovascular
Imaging Center
Bruce D. Lindsay
Cleveland Clinic Foundation of
None
None
None
None
None
None
Cardiovascular Medicine—Professor of
Cardiology
Warren J. Manning
Beth Israel Deaconess Medical Center,
■
Merck
None
None
■
Philips Medical
None
None
Division of Cardiology—Professor of
Systems*
Medicine and Radiology
Manesh R. Patel
Duke University Medical Center, Division of
None
None
None
None
None
None
Cardiology—Assistant Professor of
Medicine
Continued on the next page
APPENDIX B. CONTINUED
Institutional,
Ownership/
Organizational,
Speakers
Partnership/
or Other Financial
Expert
Participant
Employment
Consultant
Bureau
Principal
Personal Research
Benefit
Witness
Ritu Sachdeva
Emory University School of Medicine,
None
None
None
None
None
None
Children’s Health Care of Atlanta, Sibley
Heart Center Cardiology, Division of
Pediatric Cardiology, Department of
Pediatrics—Associate Professor
L. Samuel Wann
Columbia St. Mary’s Healthcare—Staff
None
None
None
None
None
None
Cardiologist
David Winchester
University of Florida, Division of
None
None
None
None
None
None
Cardiology—Assistant Professor of
Medicine
Joseph M. Allen
American College of Cardiology—Team
None
None
None
None
None
None
Leader, Clinical Policy and Pathways
Note: A standard exemption to the ACC relationship with industry policy is extended to AUC writing groups, because they do not make recommendations but rather prepare background materials and typical clinical scenarios/indications that are rated
independently by a separate panel of experts. This table represents relevant relationships of participants with industry and other entities that were reported by reviewers at the time this document was under development. The table does not necessarily
reflect relationships with industry at the time of publication. A person is deemed to have a significant interest in a business if the interest represents ownership of ≥5% of the voting stock or share of the business entity, or ownership of ≥$5,000 of the fair
market value of the business entity; or if funds received by the person from the business entity exceed 5% of the person’s gross income for the previous year. Relationships that exist with no financial benefit are also included for the purpose of
transparency. Relationships in this table are modest unless otherwise noted. Please refer to http://www.acc.org/guidelines/about-guidelines-and-clinical-documents/relationships-with-industry-policy for definitions of disclosure categories or additional
information about the ACC Disclosure Policy for Writing Committees.
*Significant relationship.
†No financial benefit.
ACC indicates American College of Cardiology; and AUC, appropriate use criteria.